
#NephJC Chat
Tuesday, May 19th, 2026, 9 pm Eastern on Bluesky and Twitter
N Engl J Med. 2026 Apr 9;394(14):1376-1387. doi: 10.1056/NEJMoa2504068.
Multifaceted Strategies for Hypertension Control in Low-Income Patients
Katherine T Mills, Marie Krousel-Wood, Erin M Peacock, Jing Chen, Farah Allouch, Amy K Carreras, Siyi Geng, Alecia Cyprian, Gerrelda Davis, Sonja R Fuqua, Darie Gilliam, Angelique Greer, Tammy Mitchell, Wylea Gray-Winfrey, Shondra Williams, Gary M Wiltz, Keith L Winfrey, Hua He, Paul K Whelton, Jiang He
PMID: 41950472
DOI: 10.1056/NEJMoa2504068





Introduction
Hypertension affects over 1.3 billion adults globally, with prevalence rising fastest in low- and middle-income countries (NCD Risk Factor Collaboration, Lancet 2021| Mills KT et al, Nature Review Nephrology, 2020). Elevated systolic blood pressure (SBP) contributed to nearly 11 million deaths in 2021 (Martin SS et al, Circulation, 2025). For every 10 mmHg reduction in SBP, there is a reduction in major cardiovascular events by 20%, stroke by 27%, and all-cause mortality by 13%- evidence that makes the persistence of uncontrolled hypertension not merely a clinical frustration, but a preventable human tragedy (Ettehad D et al, Lancet, 2016).
Yet hypertension doesn’t hurt; its silence is its cruel feature. Nonadherence to therapy is not a character flaw but rather a consequence of poverty, an architecture of chaos where daily survival consumes cognitive bandwidth. Across the globe, social determinants consistently predict worse outcomes: income-related inequalities persist even within wealthy nations like Japan, where hypertension prevalence is nearly double in low-income vs high-income groups (Aida J et al, Hypertens Res, 2024). Neighborhood deprivation drives undiagnosed hypertension in the US (River CA et al, Hypertension, 2024), and social determinants mediate one-third of the Black-White difference in uncontrolled BP (Akinyelure OP et al, Hypertension, 2023). “Clinical inertia”- failure to intensify therapy despite uncontrolled BP- compounds the problem, accounting for 40% of treatment failures in some real-world datasets (Satoh M et al, Hypertens Res, 2024).
Fig1. Possible social determinants influencing hypertension: a multilevel perspective, from Satoh M et al, Hypertens Res, 2026
Single-level strategies, when employed, have failed. A meta-analysis of 121 trials found that provider training alone yielded no significant BP reductions, while team-based care with nonphysician medication titration, health coaching, and home monitoring reduced SBP by 7.1, 3.9, and 2.7 mmHg respectively (Mills KT, Ann Intern Med, 2018). Task sharing with community health workers proved effective, even in resource-poor settings: a trial among uninsured patients in Argentina achieved a 6.6 mmHg reduction over 18 months (He J et al, JAMA, 2017). Yet Argentina’s national system bears little resemblance to the landscape of US federally qualified health centers, where insurance instability and mistrust add up to impair care. The IMPACTS-BP trial (Mills KT et al, NEJM 2026) was designed to find out whether these strategies could be employed into that uniquely challenging context- and whether intensive BP targets could be achieved safely in a low-income population.
The Study
Methods
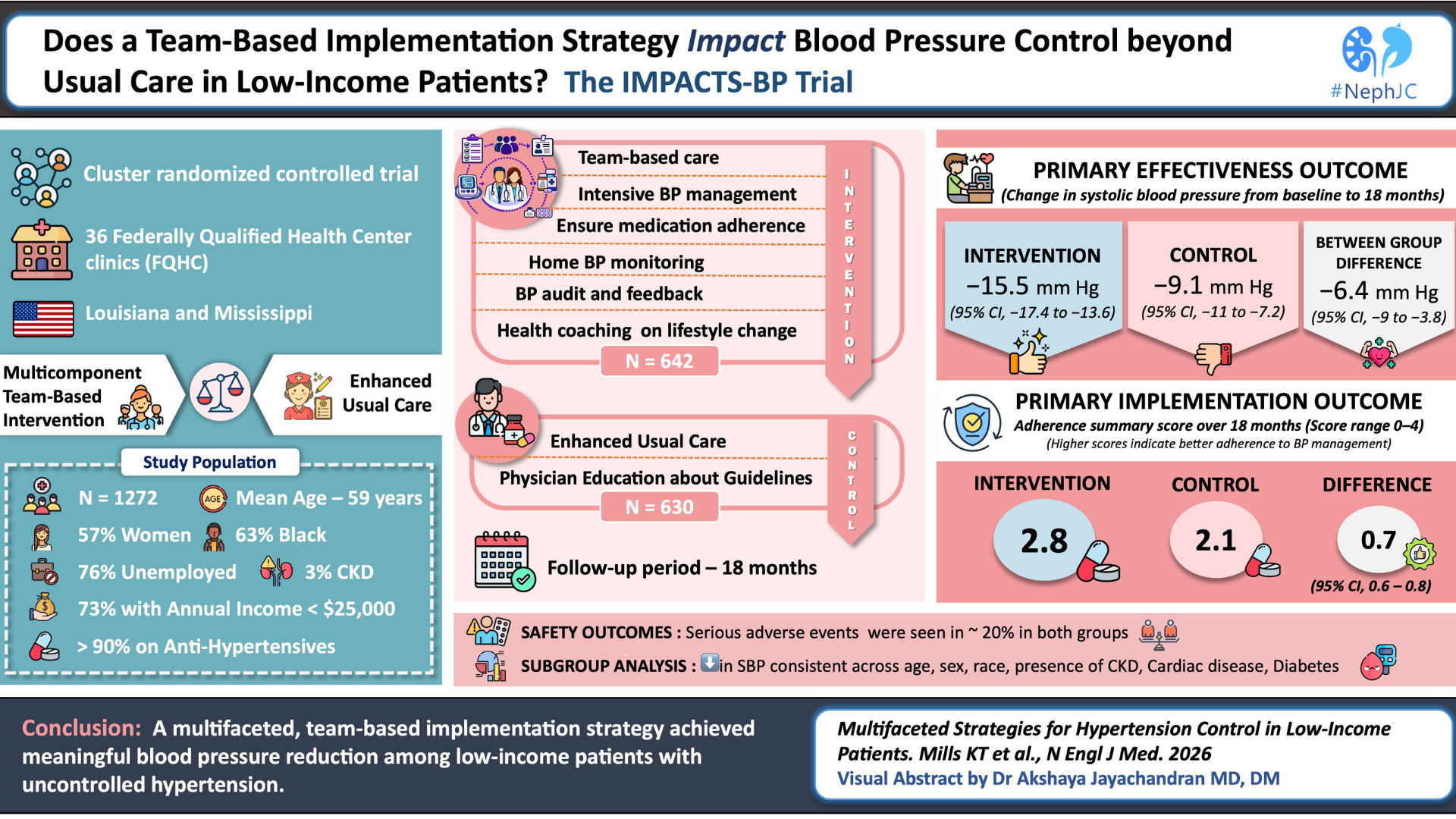
IMPACTS-BP was a cluster-randomized, effectiveness-implementation hybrid type 2 trial (Landes SJ et al, Psychiatry Res, 2019) conducted in 36 federally qualified health center (FQHC) clinics across Louisiana and Mississippi. The investigators aimed to answer 2 questions simultaneously: whether intensive hypertension treatment improves blood pressure control in underserved populations and whether resource-limited primary care clinics can realistically adopt and sustain a complex implementation strategy.
Randomization was done at the clinic level because the intervention targeted the entire care system, including providers, nurses, workflows, audit systems, and patient coaching. Clinics were randomized 1:1 to either the intervention or enhanced usual care arm, with stratification by FQHC organization to minimize imbalance between health systems.
The investigators used the Consolidated Framework for Implementation Research (CFIR) to guide both intervention development and implementation evaluation.
Figure 5. Consolidated Framework for Implementation Research, from Mills KT et al, NEJM 2026 (protocol)
Study population
Eligible participants were adults aged ≥40 years with uncontrolled hypertension and high cardiovascular risk. Participants had to have SBP ≥140 mmHg if untreated or ≥130 mmHg while receiving antihypertensive therapy. High cardiovascular risk included prior cardiovascular disease, chronic kidney disease, diabetes, estimated 10-year ACVD risk ≥10%, or age ≥65 years. Pregnant women and patients with end-stage kidney disease were excluded. Eligibility BP was confirmed using the average of six standardized measurements obtained during two screening visits.
Intervention strategy
The intervention consisted of a multifaceted, team-based implementation strategy targeting barriers to hypertension control at the system, provider, and patient levels.
The core clinical component was protocol-based intensive blood pressure management adapted from the SPRINT trial (SPRINT Research group, NEJM, 2015). The target BP was SBP <120mmHg and DBP <80 mmHg. A stepped-care algorithm guided medication intensification: if BP remained above target, providers were expected to uptitrate therapy or add another antihypertensive agent unless contraindicated.
Follow-up was intentionally intensive to reduce therapeutic inertia. Patients attended monthly visits during the first 3 months and then every 3 months thereafter; additional monthly visits continued until BP targets were achieved.
Figure S1. Antihypertensive Treatment Algorithm Modified from the SPRINT Trial, from Mills KT et al, NEJM 2026
The implementation strategy incorporated team-based care involving physicians, nurses, medical assistants, and health coaches. Staff were trained in standardized BP measurement, lifestyle counseling, and medication adherence support. All intervention patients received home BP monitors and were instructed to measure BP three days per week. Providers incorporated both clinic and home BP readings into treatment decisions. Health coaching addressed medication adherence, lifestyle modification, reminder systems, low-cost medication planning, and social barriers to care. Quarterly BP audit and feedback sessions reviewed patients with uncontrolled hypertension. Providers also underwent initial and annual retraining on intensive BP management and the SPRINT-based treatment protocol.
Control group
Enhanced usual care clinics continued routine hypertension management. Providers attended a webinar reviewing the ACC/AHA hypertension guidelines and SPRINT findings and received training in standardized BP measurement, but no additional implementation strategies were introduced.
Outcome assessment
The primary effectiveness outcome was the change in SBP from baseline to 18 months. Secondary clinical outcomes included achievement of SBP <120 mmHg, SBP <130 mmHg, reduction in SBP >30 mmHg, change in diastolic BP, quality-of-life measures, and adverse events such as hypotension, falls, and kidney function decline.
The primary implementation outcome was an adherence summary score ranging from 0 to 4. This composite incorporated four domains: high medication adherence, treatment intensification, home BP monitoring, and receipt of health education. Higher scores reflected better implementation fidelity and patient engagement.
Additional implementation outcomes included acceptability, feasibility, adoption, fidelity, sustainability, provider experience, and organizational readiness. These were assessed through surveys, electronic health records, provider assessments, and coaching completion data.
Blood pressure measurement
Blood pressure measurement was rigorously standardized. Measurements were obtained using an automated Omron HEM-907XL device with appropriate cuff sizing. Patients rested in the seated position for 5 minutes before measurements and were instructed to avoid caffeine, smoking, alcohol, and exercise for at least 30 minutes beforehand. Three BP measurements were obtained at each visit.
Statistical methods
The trial was powered to detect a 5 mmHg between-group difference in SBP, assuming an intraclass correlation coefficient of 0.063 and 20% attrition.
Missing data were addressed using multiple imputation by chained equations, generating 40 imputed datasets. The imputation model incorporated demographic variables, baseline BP, BMI, hypertension history, and cardiovascular comorbidities.
Sensitivity analyses included tipping-point analyses in which progressively worse systolic BP values were imputed into the intervention arm to determine the threshold at which statistical significance would be lost.
Funding and oversight
The study was primarily funded by the National Heart, Lung, and Blood Institute, with additional support from other NIH institutes. Oversight was provided by an independent Data and Safety Monitoring Board, and the protocol was approved by the Tulane University Institutional Review Board.
Results
A total of 1,272 participants from 36 Federally Qualified Health Center clinics across Louisiana and Mississippi underwent randomization. 642 were assigned to the multifaceted intervention strategy and 630 to enhanced usual care.
Figure 1: Enrollment, Randomization, and Follow-up from Mills KT et al, NEJM 2026
The study population reflected the communities these clinics were designed to serve - the mean age was 58.8 years, nearly two-thirds of participants were African American, over three-quarters were unemployed, and almost three-quarters reported an annual family income below $25,000. More than 90% were already receiving antihypertensive medications at baseline, and many had lived with hypertension for over a decade.
Table 1. Baseline Characteristics of the Participating Clinics and Trial Patients from Mills KT et al, NEJM 2026
Primary efficacy outcome
Over 18 months, systolic blood pressure fell substantially in both groups, although the decline was greater in the intervention arm. Mean systolic blood pressure decreased by 15.5 mmHg in the intervention group compared with 9.1 mmHg in the enhanced usual care group, yielding a net between-group difference of 6.4 mmHg. Most of this separation emerged within the first six months and was then largely sustained through follow-up. Diastolic blood pressure showed a similar pattern, with a net reduction of 3.4 mmHg favoring the intervention.
Table 2. Change in Blood Pressure over 18 Months from Mills KT et al, NEJM 2026
Secondary effectiveness outcomes
Secondary effectiveness outcomes also favored the intervention strategy. At 18 months, around 22% of patients in the intervention group and 15% in the enhanced usual care group achieved a systolic BP <120 mm Hg. Systolic BP <130 mm Hg was achieved in 48% and 36% of intervention and control patients, respectively. 18.7% of the intervention group versus 10.9% of the control group had a systolic BP reduction of >30 mm Hg from baseline. The mean reduction in diastolic blood pressure was −8.7 mm Hg in the intervention arm compared with −5.3 mm Hg in the control arm, with a between-group difference of −3.4 mm Hg. Changes in physical and mental SF-12 quality-of-life scores were similar between groups.
Table 2. Effectiveness, Implementation, and Adverse Outcomes, from from Mills KT et al, NEJM 2026
The results were robust across sensitivity analyses. The complete case analysis, which included only patients with complete data, showed an even larger effect: -16.1 mmHg in the intervention group vs -9 mmHg in controls, yielding a between-group difference of -7.1 mmHg (95% CI, -9.7 to -4.4). The tipping point analysis (table S8) demonstrated that missing data would need to be inflated by +6.5 mmHg in the intervention group before the result lost statistical significance, confirming the robustness of the primary finding.
In the subgroup analysis, the intervention appeared to work similarly across age groups, in both men and women, among Black and non-Black participants, and across different levels of income, education, and insurance status. It also showed similar benefits in participants with and without cardiovascular disease, diabetes, or chronic kidney disease. The magnitude of reduction varied slightly between groups, however there was no clear evidence that the intervention worked substantially better or worse in any particular subgroup. Sensitivity analyses, including complete-case and tipping-point analyses, did not materially alter the primary findings.
Figure 3: Between-Group Difference in the Change in Systolic Blood Pressure over 18 Months According to Subgroup from Mills KT et al, NEJM 2026
Implementation outcomes
Implementation outcomes favored the intervention group throughout the trial. The trial showed that the fidelity scores (which reflect adherence to major intervention components like medication intensification, home BP monitoring, and health coaching) were consistently higher in the intervention clinics. Treatment intensification occurred in more than 90% of intervention participants compared with 71.5% in the control arm, and home blood pressure monitoring was nearly universal in the intervention group. Interestingly, self-reported medication adherence did not significantly differ between groups despite the greater blood pressure reduction observed in the intervention arm.
Another noteworthy point is that, over the course of follow-up, the rates of both provider and health coaching visit completion decreased. Health coaching visit completion reduced from 94.1% at baseline to 53.4% at 3 months and then fluctuated between 43% and 66% during later follow-up visits. A similar pattern was observed for provider visits, with completion rates falling from 87.1% at baseline to 52.2% at 3 months and remaining between 40% and 56% thereafter.
Figure S5. Proportion of Completed Provider and Health Coach Visits During the18-Month Intervention from Mills KT et al, NEJM 2026
Serious adverse events were seen in both groups with similar frequencies of around 20%. There wasn’t a significantly increased frequency of hypotension, syncope, falls, or kidney-related adverse events in the intervention arm.
Discussion
At first glance, this trial appears to be about blood pressure reduction, but the more one sits with the paper, the clearer it becomes that the intervention was not simply the intensification of drugs. It was about the restructuring of care. The discussion of any trial usually focuses on the trial methodology, the results, and if the “significant” values were actually significant. However, this trial gives us an entirely different direction of discussion. In a single word: implementation.
The investigators did not try out a novel drug or some breakthrough biologic pathway. They simply tried to redesign/reframe the rules surrounding hypertension management. BP was just measured more carefully, reviewed more frequently, discussed more consistently, and acted upon more aggressively. They coached, followed, and reminded the patients, and the patients were drawn into the process through home monitoring and repeated engagement. The study asked a question which seems deceptively simple: what happens when vulnerable patients receive the kind of organized hypertension care that guidelines assume already exists?
The answer? A 6.4 mmHg greater reduction in systolic blood pressure. This is not a trivial finding, more so because the population was already heavily treated at baseline. It’s also notable that the benefit was achieved in an underserved population frequently excluded from tightly controlled efficacy trials: predominantly low-income patients who receive care in resource-limited settings. These are places where factors such as therapeutic inertia, fragmented follow-up, and multiple other barriers dominate everyday practice more than drugs and doctors do.
Notably, IMPACT-BP’s impact isn't an isolated one. Previous community-based hypertension studies have shown that even relatively simple, culturally grounded interventions can produce meaningful improvements in BP control when it is accessible and persistent. The landmark “barbershop trial” among Black men (Victor RG et al, NEJM 2018) is perhaps the best example of this, where blood pressure reduction was achieved by combining trusted community spaces with pharmacist-led medication management.
So we are led to believe that a multipronged strategy = BP lowering in low-resource settings. Case closed. And yet, the study becomes more interesting as we think further and deeper.
The control group also had nearly 9 mmHg reduction in systolic BP, and this points us towards a simple fact. Medical attention, by itself, is therapeutic. Standardized BP measurement, education of the healthcare providers, repeated follow-up, and participation in a trial most likely improved care even in those who didn't get the full intervention package. What does this mean? This makes the between-group difference more credible, but it also highlights how poorly measured BP, in conjunction with irregular follow-up, may contribute to apparent “treatment-resistant” hypertension in routine practice.
A key observation is that the intervention arm had meaningful BP reduction even though the medication adherence wasn’t significantly better. This disconnect raises huge questions. Was the scale used (Morisky Adherence Scale) simply too blunt to capture the real behavioral change? Did the medication intensification protocol overcome the not-so-good adherence? Or is self-reported adherence fundamentally unreliable? These are the socially vulnerable populations where medication-taking behaviour is fluid. Does this factor make adherence hard to measure? The trial does not fully answer this, but it shows that there are many factors apart from patient-reported drug adherence that lead to BP control.
This trial also exposes the persistent discord between evidence and implementation. Although the intervention was modeled after SPRINT-style intensive BP control, fewer than 1/4th of participants ultimately achieved a systolic BP below 120 mmHg. The authors suggest that providers may have hesitated to pursue such aggressive targets because there are quality benchmarks in Federally Qualified Health Centers that still emphasize less stringent thresholds. This, in itself, shows that there is a wide gap between what guidelines recommend, what doctors practice, and what is best for any individual patient. While trials increasingly support lower BP targets, individualized BP goals will always eclipse population-based goals.
Although the results seem overwhelmingly favorable towards the intensive strategy, we have to be cautious about certain points. This was a bundled intervention, making it impossible to determine which component carried the greatest weight. Was it home BP monitoring or the health coaching? Audit and feedback? Medication intensification? Or simply more human contact? The intervention succeeded as a package, but the ability to scale it may depend on knowing which pieces are essential and which are merely supportive. At the end of the day a more selective approach may be more cost-effective and generalizable.
From a nephrologist’s perspective, there was a small proportion of participants with CKD in the trial. This limits direct extrapolation to higher-risk CKD populations. Also, hypertension management in CKD is often complicated by volume overload, polypharmacy, fluctuating kidney function, and competing cardiovascular risks. Although the subgroup analyses were consistent, the study was not specifically designed to answer whether these implementation strategies perform similarly in patients with advanced kidney disease.
Whatever is said and done, the crux of hypertension management is the drugs we use to control BP. Interestingly, there are no data regarding the choice and sequence of drugs used and how many percent of the trial population that received each drug, and at what dose. That would have added more scientific rigor and guidance from this implementation study.
Another issue is with the sustainability of this package. This intervention was done within the structured plan of a fully funded clinical trial, and yet the provider and health coach visit completion rates significantly declined over time. The average implementation cost approached $760 per participant, which may appear reasonable from a public health perspective, but is pretty challenging for under-resourced primary care systems already operating under financial strain. Finally, this study was only 18 months, what kind of intensity and expense would be expected over potentially decades (a lifetime) of treatment? The trial proves that intensive hypertension management can work in low-income populations. Whether health systems are willing to invest in maintaining that intensity is a separate question entirely.
Conclusion
IMPACT-BP showed that meaningful blood pressure reduction is possible in underserved populations when provided with structured, consistent, and team-based care. At the same time, it reminds us that sustaining this level of intensity of care outside a clinical trial remains challenging.
Summary by
Akshaya Jayachandran
Cristina Popa
Reviewed by
Brian Rifkin, Swapnil Hiremath
Header Image created by AI, based on prompts by Cristina Popa