
N Engl J Med, May 14, 2026 DOI: 10.1056/NEJMoa2514415
Telitacicept for IgA Nephropathy - Interim Analysis of a Phase 3 Trial
Jicheng Lv, M.D., Lijun Liu, M.D., Wenxiang Wang, Ph.D., Xinyue Wang, Ph.D.,Qing Zuraw, M.D., Vlado Perkovic, M.D., Ph.D., Jianmin Fang, Ph.D.,and Hong Zhang, M.D., Ph.D., for the TELIGAN Investigators
PMID: 42127391
DOI:10.1056/nejmoa2514415
Why was this study needed?
We’re at quite an interesting juncture in IgAN therapeutics. Five years ago, we were still debating what dose of steroids should remain in the conversation after TESTING | (NephJC Summary). Today, the challenge is almost the opposite: there are so many promising therapies that reduce proteinuria, and the question is which drug to select and which pathway to target for which patient.
We’ve seen targeted-release budesonide (NefIgArd) | (NephJC Summary) focus on the gut mucosal immune system. Complement inhibition entered the scene with Iptacopan (APPLAUSE - IgAN) | (NephJC). More recently, APRIL-directed therapies such as sibeprenlimab (VISIONARY) | (NephJC Summary) and atacicept (which is dual BAFF-APRIL, ORIGIN) | (NephJC Summary | Podcast) have delivered striking reductions in proteinuria. Telitacicept now joins this increasingly crowded field, sharing the distinct biological proposition of atacicept: simultaneous blockade of both BAFF and APRIL rather than targeting either pathway alone.
Infographic on Trials in IgA Nephropathy by Cristina Popa
With a slew of drugs already approved for IGAN, why does this trial matter?
BAFF and APRIL signaling sit in the space of B-cell survival, plasma-cell maturation, and immunoglobulin production. Elevated levels of both cytokines have been linked to IgAN activity. Telitacicept is essentially a soluble TACI-Fc fusion protein that acts as a decoy receptor, binding both BAFF and APRIL simultaneously. Theoretically, this should reduce production of pathogenic galactose-deficient IgA1 and downstream immune complex formation. The TELIGAN trial asks a direct question - exactly the same as with ORIGIN (atacicept): can dual BAFF/APRIL inhibition meaningfully alter disease activity (in the form of proteinuria and GFR stabilization) in high-risk IgAN? This question has been asked and answered for various groups of drugs in IgAN. After atacicept, do we need another -tacicept? Why not - the more the merrier! So, hit me baby one more time.
Fig. 1: Role of telitacicept in the treatment of IgA nephropathy from Wu, L. et al. Eur J Med 2023
How was the study done and what did it find?
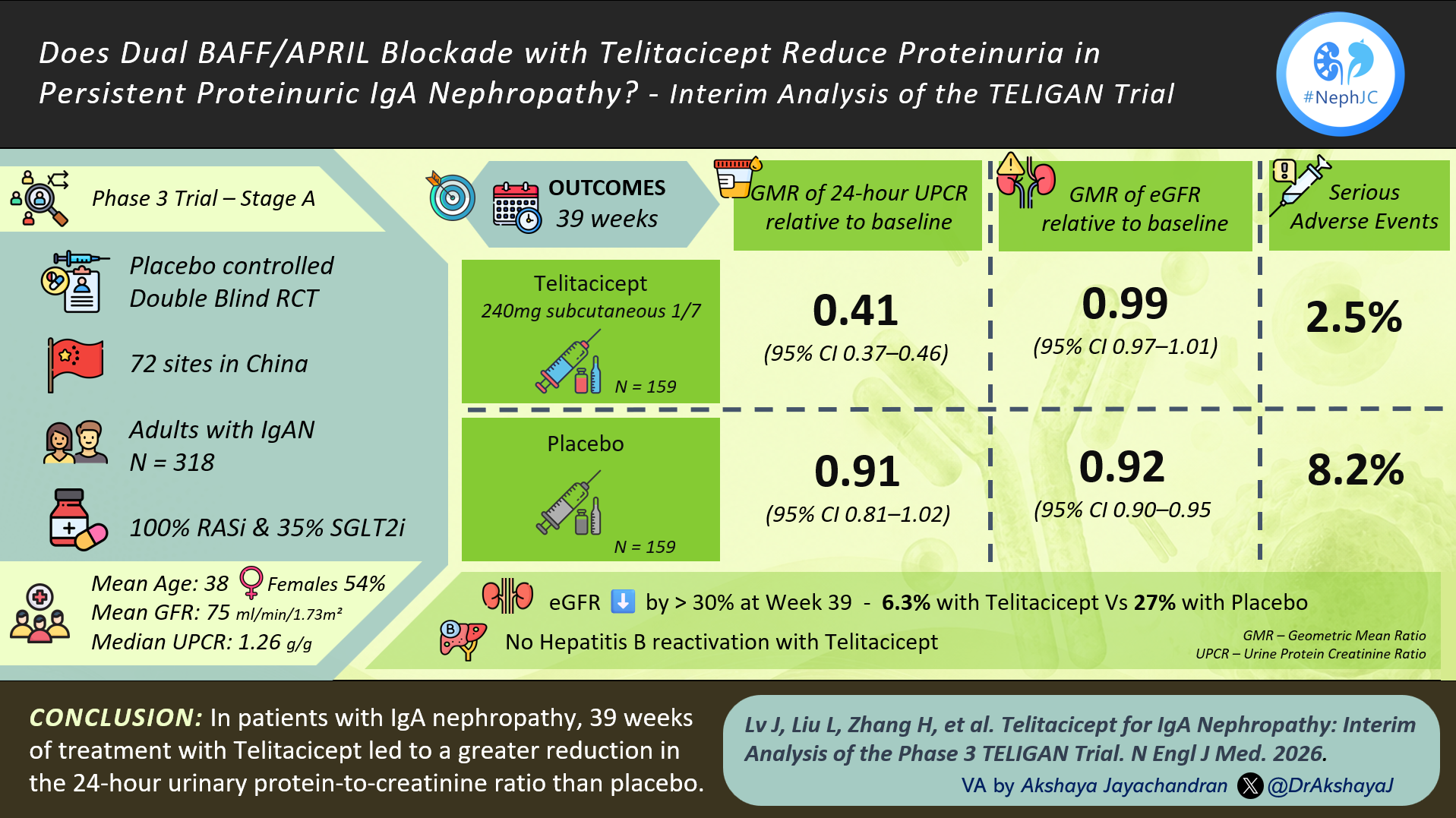
TELIGAN is a phase 3, multicentre, double-blind, placebo-controlled study conducted across 72 centres in China. They included adults with biopsy-proven IgAN, UPCR ≥0.5 g/g, eGFR ≥30 mL/min/1.73 m², and persistent proteinuria despite ≥12 weeks of maximally tolerated RAS blockade. This paper represents a prespecified interim analysis (stage A) focused on proteinuria at 39 weeks, while the ongoing stage B will evaluate longer-term kidney function outcomes through 104 weeks. The trial is being funded by Remegen (the company manufacturing telitacicept). If you have read any of the IgAN trials linked above, feel free to skip the methods, they are almost a CTRL-C/CTRL-V of each other.
Figure 1: Study design from J Lv et al, NEJM 2026
A total of 318 adults with biopsy-proven IgAN were randomized 1:1 to weekly subcutaneous telitacicept 240 mg or placebo on a background of standard of care. Patients had persistent proteinuria despite optimized Renin Angiotensin System(RAS) blockade, eGFR ≥30 ml/min/1.73m², and were not receiving glucocorticoids or other immunosuppressive therapies. About one-third were already flozinated, reflecting contemporary practice. Unlike RAS blockade, flozination was allowed, but not required as part of standard of care.
The primary endpoint for this analysis was reduction in 24-hour urinary protein-creatinine ratio at week 39.
What were the results?
Figure S1. Screening, Randomization, and Follow-up, from J Lv et al, NEJM 2026
The mean age was 38 years, with women comprising just over 50% of the study population. Mean eGFR was around 75 mL/min/1.73 m², and the median baseline 24-hour urinary protein-to-creatinine ratio was 1.26 g/g. Approximately 1/3rd of participants had eGFR < 60 mL/min/1.73 m². Histologic characteristics showed M1 lesions present in ~79% and crescents (C1/C2) in ~45% of patients with available biopsy data. Around 70% had hematuria. All patients were receiving background RAS blockade at randomization.
Table 1. Demographic and Clinical Characteristics of the Patients at Baseline from J Lv et al, NEJM 2026
At 39 weeks, proteinuria fell by 58.9% with telitacicept compared with only 8.8% with placebo, with a relative treatment effect of −55% (95% CI −61.3 to −47.6; P<0.001). Separation from placebo appeared as early as week 4 and continued to widen over time. Equally striking was the proportion achieving a UPCR below 0.8 g/g: 61% with telitacicept versus only 19.5% with placebo.
Figure 1. Changes in 24-Hour Urinary Protein-to-Creatinine Ratio over a Period of 39 Weeks from J Lv et al, NEJM 2026
Mean eGFR was essentially preserved in the telitacicept group (−1.0%) while declining in the placebo arm (−7.7%) over 39 weeks. Likewise, fewer patients experienced a ≥30% eGFR decline (6.3% vs 27%). Interestingly - in China they are allowed to present GFR data at this stage (you may note that the ORIGIN atacicept phase 3 trial suppressed that - the FDA only allows that to be analysed at 2 years).
Figure 2. Changes in Estimated Glomerular Filtration Rate (GFR) over a Period of 39 Weeks from J Lv et al, NEJM 2026
The clinical response was also accompanied by pharmacodynamic effects. Circulating CD19-positive B cells fell by nearly 50%, while immunoglobulin levels declined substantially. Serum IgA levels decreased by approximately 60%, supporting the notion that the drug is engaging the intended disease pathway.
Figure S8. Pharmacodynamic Effects on B-cells and Immunoglobulins from J Lv et al, NEJM 2026
The overall adverse event rate was higher with telitacicept (89% vs 79%), largely driven by injection-site reactions and expected immunoglobulin reductions. Serious adverse events were actually less frequent with Telitacicept (2.5% vs 8.2%). Infection rates were broadly similar between groups. No deaths occurred. With regard to the HBV data, among 68 patients with latent hepatitis B infection, no reactivation occurred in those receiving Telitacicept during the 39-week study period. For clinicians practicing in Asia, where latent HBV is common, this is clinically relevant, although the sample size and follow up remains modest at this time.
WHAT ARE THE IMPLICATIONS?
TELIGAN shows that telitacicept produces one of the greatest reductions in proteinuria seen in contemporary IgAN therapeutics - similar to what was seen with sibeprenlimab and atacicept. The effect is consistent across subgroups, appears within four weeks, and is accompanied by reductions in circulating B cells, immunoglobulins and serum IgA, engaging a central pathogenic pathway in IgA nephropathy. This is also supported by the fall in hematuria (post-hoc analysis) from ~71% to ~21% with telitacicept and essentially unchanged with placebo. This matters because proteinuria can improve through hemodynamic mechanisms, but hematuria is often considered a marker of active glomerular inflammation, and since telitacicept improves both, it could be a disease-modifying effect. Given all these strengths, the enthusiasm generated by TELIGAN is understandable
This remains a short term proteinuria reduction data report however (like all recent IgAN trials). The kidney function data are encouraging but shouldn’t be overinterpreted. The apparent eGFR preservation and lower frequency of a 30% eGFR fall favour telitacicept, but these were secondary analyses, the study was not powered for kidney outcomes and is just an interesting sidenote - we have to await 2 year GFR data (same as with other IgAN new therapeutics).
When we compare it with other phase 3 IgAN trials, we get an interesting context. Unlike ORIGIN, VISIONARY and APPLAUSE-IgAN, which enrolled multinational cohorts, TELIGAN was conducted exclusively in a Chinese population. Patients in TELIGAN were randomized a median of more than four years after biopsy, compared with around 2.5 years in ORIGIN and 1.5 years in VISIONARY and APPLAUSE-IgAN.
Baseline proteinuria was among the lowest across these studies (median UPCR ~1.3 g/g in TELIGAN and VISIONARY, ~1.9 g/g in APPLAUSE-IgAN, and ~2.2 g/g in ORIGIN). Also, this was also a well-treated cohort - with baseline standard of care similar to other IgAN trials (with supportive/palliative therapies). All patients received optimized RAS blockade and 35% were already receiving SGLT2 inhibitors, compared with 50% in ORIGIN, 40% in VISIONARY and 12% in APPLAUSE-IgAN. This suggests that the study population consisted of patients with established, persistent IgAN.
Again, with established disease and already on baseline RASi/ some SGLT2i, the placebo arm still achieved an 8.8% fall in proteinuria. The numerically greater decrease in proteinuria with telitacicept than all other trials cannot be signal - comparing across studies with heterogeneous populations is fraught with uncertainty.
At present, it is difficult to know whether dual BAFF/APRIL blockade represents a genuine therapeutic advance over selective APRIL inhibition or simply another effective approach targeting the same biological pathway. As direct comparative trials are unlikely until several years from now, this question will probably be answered gradually through accumulating clinical experience and longer-term outcome data. While telitacicept may (or may not) make it to European or North American populations - would Chinese pharmaceutical companies be interested in making these drugs available in other parts of the world - especially across Asia where IgAN is so prevalent and where only steroids are available so far? Will they make it cheaper than sibeprenlimab, atacicept et al? One can hope.
BOTTOMLINE?
TELIGAN is a well designed phase 3 study that delivers a remarkably consistent and biologically plausible treatment signal. The magnitude of proteinuria reduction is among the largest reported in IgAN, seems to have a convincing target engagement, and the short term safety profile appears acceptable
By
Reviewed by