
#NephJC Chat
Tuesday, September 16th, 2025, 9 pm Eastern on Bluesky
Circulation. 2025 Aug 14. doi: 10.1161/HYP.0000000000000249. Online ahead of print.
2025AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/ AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines
Daniel W Jones, Keith C Ferdinand, Sandra J Taler, Heather M Johnson, Daichi Shimbo, Marwah Abdalla, M Martine Altieri, Nisha Bansal, Natalie A Bello, Adam P Bress, Jocelyn Carter, Jordana B Cohen, Karen J Collins, Yvonne Commodore-Mensah, Leslie L Davis, Brent Egan, Sadiya S Khan, Donald M Lloyd-Jones, Bernadette Mazurek Melnyk, Eva A Mistry, Modele O Ogunniyi, Stacey L Schott, Sidney C Smith Jr, Amy W Talbot, Wanpen Vongpatanasin, Karol E Watson, Paul K Whelton, Jeff D Williamson
PMID: 40811516






Introduction
Hypertension guidelines don’t roll out every year, and in the hypertension timeline, 2017 feels ancient. That was the last big shake-up, when the AHA/ACC dropped the threshold of defining hypertension to ≥130/80 mm Hg (Whelton et al, JACC 2017), a move anchored in SPRINT (SPRINT Research Group, NEJM 2015) and the countless debates that followed. The NephJC team addressed this shift in a 2017 NephJC summary, when the new cut-off reclassified millions of individuals and reshaped the conversation around diagnosis and treatment. Before diving in, it helps to frame the problem. Hypertension remains the most common – and arguably the most stubborn – modifiable risk factor for cardiovascular disease. More than a billion people worldwide live with it (O’Connell et al, Circulation, 2025), and in many countries that translates to about one in three adults. In the US, from 2017 to 2020, the prevalence was 46.7%.
Table from Jones et al, Circulation 2025
We’ve had effective therapies for decades, yet control rates remain unacceptably low, particularly in low- and middle-income settings (Mishra et al, Hypertension 2025). Globally, an estimated 1.28 billion adults aged 30–79 years are living with hypertension, and nearly half are unaware of their diagnosis (Zhou et al, Lancet 2021). And while the conversation often centers on the heart, the burden is far broader: kidneys, brain, and vessels all share the damage. Hypertension isn’t just a number on a chart – it’s the quintessential multisystem disruptor. Fast forward to 2025, the numbers haven’t budged, but the perspective has.
Table from Jones et al, Circulation 2025
The 2025 update emphasizes risk-based management, kidney-focused detection, and an expanding toolkit that extends well beyond the office cuff (Jones et al, Circulation 2025). Consistent with prior documents, the ACC/AHA continues to employ the framework of “Class of Recommendation” and “Level of Evidence”, aligning each intervention or diagnostic strategy with both its strength of recommendation and the quality of supporting data.
Table from Jones et al, Circulation 2025
The full update is an extensive and encyclopedic beast; so for everyone’s sanity, consider this our curated tour of the highlights that matter most.
2017 vs 2025: What’s Changed
The 2017 AHA/ACC hypertension guideline was nothing short of disruptive—arguably the most consequential shift in blood pressure management since JNC 7 in 2003 (Muntner et al, Circulation 2017). By redefining hypertension as ≥130/80 mm Hg, it expanded prevalence in the U.S. from about 32% to 46% of adults, affecting nearly 116 million people. Overnight, millions who had been labeled “pre-hypertensive” were now formally “hypertensive”, with implications not just for treatment decisions but for insurance coverage, patient identity, and public health strategies.
Figure from Muntner et al. Circulation 2018
This seismic shift was anchored in the SPRINT trial in 2015, which randomized >9,000 high-risk, non-diabetic adults to intensive (<120 mm Hg) vs standard (<140 mm Hg) systolic targets (SPRINT Research Group, NEJM 2015). Intensive control reduced the composite of myocardial infarction, other ACS, stroke, heart failure, or cardiovascular death by 25%, and all-cause mortality by 27%. A subsequent meta-analysis (Ettehad et al, Lancet 2015) reinforced a linear, continuous relationship between blood pressure and CV risk, starting as low as 115/75 mm Hg.
Figure from SPRINT Research Group, NEJM 2015
But the 2017 guideline was not without controversy. Critics argued it risked overdiagnosis and overtreatment, particularly in lower-risk populations, and raised concerns about the feasibility of widespread implementation. Still, the message was clear: cardiovascular risk accumulates well before 140/90, and waiting until then to intervene was too late.
Fast forward to 2025, and the new AHA/ACC guideline holds the line on ≥130/80 mm Hg—a signal that the evidence since 2017 has only strengthened that position. But the focus has shifted. Where 2017 asked, “Who has hypertension?”, now 2025 asks, “How do we best detect, stratify, and manage it?”
Key differences now include fourteen class 1, three class 2A and three class 3 new recommendations:
Terminology shift: The outdated term hypertensive urgency is retired, replaced by severe hypertension without acute target-organ damage, to better reflect pathophysiology and avoid unnecessary ED visits and admissions. For these patients, the emphasis is not on aggressive short-term BP lowering or IV drugs, but on restarting or intensifying oral therapy, ideally as an outpatient.
Adoption of the PREVENT calculator and incorporating outcomes such as heart failure, CVD and ASCVD
Routine albuminuria testing now recommended for all patients with hypertension, elevating CKD from an afterthought to a core component of cardiac-kidney-metabolic risk assessment.
Secondary hypertension is emphasized with broader, stronger recommendations for screening, particularly for primary aldosteronism.
Beyond MI and stroke, the guideline recognizes hypertension’s role in heart failure, CKD progression, and cognitive decline.
In short: 2017 redefined hypertension; 2025 redefines hypertension care.
Risk Assessment Gets an Upgrade
One of the most notable changes is the replacement of the Pooled Cohort Equations (PCE) with the PREVENT risk framework for clinical risk assessment. The original PCE (2013) estimated 10-year ASCVD risk but has well-documented calibration issues (Campos-Staffico et al, Atherosclerosis 2021) in some populations and does not capture non-ASCVD outcomes such as heart failure and kidney disease.
Visual abstract from Campos-Staffico et al, Atherosclerosis 2021
{kind=link}
The PREVENT equations and calculator (Khan et al, Circulation 2023) were developed to address these gaps. They use contemporary, diverse U.S. cohorts, allow additional optional inputs such as urine albumin-creatinine ratio (UACR), HbA1c, and social deprivation index, and provide both 10-year and 30-year (lifetime) risk estimates for multiple outcomes, including ASCVD, heart failure, and stroke.
Figure from Khan et al, Circulation 2023
The AHA/ACC now recommends PREVENT to inform treatment decisions for stage 1 hypertension, reflecting a shift from short-term ASCVD probability toward multi-organ, lifetime risk assessment. This is a deliberate reframing: hypertension management is becoming risk-based, not number-based. Instead of focusing solely on whether a patient crosses the ≥130/80 mm Hg threshold, clinicians are now asked to consider overall multi-organ risk, including cardiovascular, renal, and cognitive endpoints. That said, PREVENT raises practical questions—complexity for point-of-care use, external validity outside U.S. cohorts, and whether albuminuria and other kidney-specific signals receive adequate weight in risk estimates. Validation and performance studies are emerging, but clinicians and nephrologists should be attentive to how PREVENT performs in CKD subgroups and diverse practice settings.
Figure from Jones et al, Circulation 2025
Kidneys Step Into the Spotlight
Hypertension and kidney disease exist in a vicious cycle. Elevated blood pressure accelerates CKD progression, and worsening kidney function, in turn, exacerbates hypertension and amplifies cardiovascular risk. The 2025 AHA/ACC guideline recognizes this interplay and introduces several key updates that significantly enhance the role of nephrologists in managing hypertension.
A major recommendation is routine albuminuria screening for all patients with hypertension, using UACR. Albuminuria is not only a sensitive marker of early kidney damage but also a strong, independent predictor of cardiovascular events, aligning with KDIGO’s 2021 (KDIGO Blood Pressure Work Group, Kidney International 2021) guidance on CKD risk stratification. Incorporating albuminuria into risk assessment is another important update. Alongside eGFR, albuminuria feeds into the PREVENT calculator, refining lifetime risk estimates for both kidney and cardiovascular outcomes. These measures determine treatment intensity, particularly for high-risk patients, ensuring that therapy is tailored to both cardiovascular and renal risk.
For patients with CKD and albuminuria, intensive blood pressure control (target <130/80 mmHg) is strongly recommended, with ACE inhibitors or ARBs preferred when proteinuria is present. Early identification and intervention allow timely nephrology referral and prevent cardiovascular complications (SPRINT Research Group, NEJM 2015). Overall, the guideline elevates kidney outcomes from a secondary consideration to a primary driver of management decisions, marking a paradigm shift in which nephrologists can advocate for albuminuria-guided hypertension care as a standard approach.
Table from Jones et al, Circulation 2025
Secondary Hypertension Gets Serious
Much is new regarding secondary hypertension, especially a comprehensive list of whom to screen and how.
One previously discussed topic is the screening and treatment of primary aldosteronism (NephJC|summary). Although a common cause of secondary hypertension (up to 20% of patients with resistant hypertension), screening sits at an abysmal low, even in a high risk population (Cohen et al, Ann Intern Med. 2021, Mulatero et al, J. Hypertension 2016), owing a lot to the absence of hypokalemia in a significant fraction. A potential fatal oversight seeing as the rate of renal (Monticone et al, Journal of Hypertension 2020) as well as cardiovascular (Monticone et al, Lancet 2018) complications is significantly higher in this patient group.
The most important change in the recommendations is that screening is extended to patients with resistant hypertension without hypokalemia (class 1) but also in everyone with stage 2 hypertension (BP > 140/90, level 2b). This has already been addressed in the most recent clinical guidelines by the Endocrine Society (Adler et al, JCEM 2025) and aligns with the 2024 ESC Hypertension Guideline (McEvoy et al, EHJ 2024) from last year. The Endocrine Society, of course, take it a step further than the AHA/ACC and ESC guidelines and recommend screening everyone with hypertension for primary aldosteronism.
Figure from Jones et al, Circulation 2025
That the kidney is now in the spotlight has already been addressed above, but other therapeutically relevant causes, such as OSA, drug induced and endocrine disorders have been duly considered with clear recommendations for screening.
Targets and Thresholds: No Moving Targets
We seem to be staying at the same threshold of 130 mmHg SBP as the dividing line, with the small addition that in patients with heightened CVD-risk, meaning a PREVENT-Score of >7.5%, a goal BP of 120 mmHg SBP is “encouraged”. This is recommended mainly on the basis of the BPROAD (Bi et al, NEJM 2024) and ESPRIT-Trials (Liu et al, Lancet 2024) showing a benefit for intensive BP-control regardless of patient comorbidities like diabetes.
Table from Jones et al, Circulation 2025
In general we are moving increasingly to individualized risk assessment and treatment decisions with the PREVENT-Score, as well as concomitant diseases such as CKD, DM, CVD, HF and many more. A very significant new recommendation in the context of resistant hypertension, defined as uncontrolled hypertension under optimal treatment with first line agents (ACEi/ARB, thiazide-like diuretics and CCBs), the addition of MRAs is recommended in all patients without contraindications.
One point of critique in 2017 was the extrapolation of data from the SPRINT-Trial to a lower risk collective in the guidelines. While this has been addressed through the PREVENT-Score, the limitation remains that the guideline largely relies on the same data from SPRINT.
Orthostatic hypotension, especially in elderly and frail people, is a consideration that often leads to less intensive BP-lowering in clinical practice but there is a clear I A recommendation that an improved BP-control leads to a decrease in CVD-risk without an increased risk in falls, shown in the SPRINT-, CRHCP- and NAILED-trial.(Ögren et al, PLoS One 2024).
There are more added practice recommendations sprinkled throughout:
A stepped-care approach is reasonable in older adults instead of the SPC
Alpha-blockers and sodium nitroprusside should be used with caution due to increased unwanted side effects
Aerobic exercise and salt-restricted diets are effective in elderly patients
Beyond the Cuff: Expanding the Scope
In a positive development, this guideline addresses patient centered factors like social determinants of health and optimization of adherence. Additionally, it expands on the cornerstone of lifestyle modifications with the addition of potassium-based salt substitution and potassium-rich diet. There have been a number of interesting trials looking at this on a larger scale (e.g. Neal et al, NEJM 2021), and a very good NephJC Blog, showing a consistent reduction in systolic BP. In the current guideline the recommendation excludes patients with CKD, something a nephrologist might take a less cautious approach on recommending to patients with advanced CKD (Ramos et al, NDT 2020)(Morimoto et al, Renal Nutrition 2024), although the evidence for a beneficial BP effect in that group is a lot more questionable (Turban et al, Nutrients 2021).
Table from Jones et al, Circulation 2025
Coming more into focus is the therapy of obesity, and the importance of weight reduction in the treatment of hypertension a new recommendation here is the use of GLP-1-receptor agonists and other incretin-mimetics as adjunct therapy in obesity.
Figure from Jones et al, Circulation 2025
To combat treatment adherence, and gaps in access to care, the recommendations include a team-based community approach. Alignment with social group structures like churches, social workers and community leaders is encouraged to facilitate increased awareness. In order to increase ease of access, the use of home measurements and electronic devices for improved contact and out-of-office monitoring are also recommended. Unfortunately, widespread adoption and implementation of these measures seems unlikely due to a lack of a reimbursement structure.
There are a multitude of smaller interesting new recommendations and aspects we cannot cover, but here is one more of interest.
The upgraded Level I A recommendation for BP control to reduce cognition impairment and dementia. A connection that was shown in the SPRINT-MIND (Williamson et al, JAMA 2019) follow-up trial, as well as in CRHCP (He et al, Lancet 2023).
Pregnancy Matters
Another area where we had a lot of new evidence appear between 2017 and now is with regard to pregnancy related hypertension and associated complications, like preeclampsia. The new treatment threshold of <140/90mmHg for hypertension in pregnancy based on the CHAP-Trial (Tita et al, NEJM 2022), discussed with all its strengths and limitations in a prior NephJC. Another change is the choice of preferred antihypertensive medication in pregnancy being labetalol and long extended-release nifedipine, stepping away from the prior first choice agent methyldopa (Abalos et al, Cochrane Database Syst. Rev. 2018)
Visual abstract, Anand Chellapan, NephJC 2022
The second important new recommendation is for a prophylactic daily low dose aspirin therapy in patients at risk for preeclampsia, lowering the risk of of perinatal mortality, preterm birth and small for gestational age/intrauterine growth restriction (Henderson et al, Evidence Synthesis 2021)
Renal Denervation: Where Do We Stand
If lifestyle modifications, pills, and drug combinations are still the bedrock of hypertension care, device-based therapies are creeping closer to center stage. At the forefront is renal denervation (RDN), a catheter-based method that disrupts renal sympathetic nerve activity to lower blood pressure.
Visual abstract by Carlos Trinidad, AJKD 2025
So where does RDN stand in 2025? The AHA/ACC guidelines acknowledge it, but with caution. Since the underwhelming results of SYMPLICITY HTN-3 (Bhatt et al, NEJM 2014), newer sham-controlled trials such as RADIANCE-HTN TRIO (Azizi et al, Lancet 2021) and SPYRAL HTN-ON MED (Böhm et al, Lancet 2020) have shown modest but consistent BP reductions (NephJC Summary). That said, questions about long-term durability, patient selection, safety, and cost remain. Check the NephMadness summary and commentary for more (Torres, AJKD 2025 and Hiremath, AJKD 2025).
Who might benefit? According to the guidelines, RDN may be considered in carefully selected patients: those with both systolic and diastolic hypertension (office SBP 140–180 mm Hg and DBP ≥90 mm Hg) and preserved kidney function (eGFR ≥40 mL/min/1.73 m²). This applies to individuals with resistant hypertension despite optimal therapy, or those who cannot tolerate further medication escalation. It is not a replacement for medications but might serve as an adjunct in resistant cases.
Table from Jones et al, Circulation 2025
The 2025 AHA/ACC guidelines finally gave RDN a seat at the table with a Class IIb recommendation, but access in the U.S. is still a work in progress. FDA approval came through in November 2023, with Medtronic’s Symplicity Spyral and Recor’s Paradise ultrasound systems officially cleared for clinical use (Beck, Cardiology 2024). Meanwhile, CMS has proposed coverage under Coverage with Evidence Development for patients with uncontrolled hypertension who meet guideline criteria. In other words: the guidelines say “yes,” the FDA says “go,” but insurers haven’t fully RSVP’d yet.
Reframing Severe Asymptomatic Hypertension
One of the more striking shifts in the 2025 AHA/ACC guidelines isn’t about thresholds or targets—it’s about terminology. The outdated label “hypertensive urgency” has officially been retired. In its place, the more precise phrase severe hypertension without acute target-organ damage is used—better reflecting underlying pathophysiology and helping avoid unnecessary emergency department visits, aggressive IV therapy, and provider/patient anxiety.
Why the change? The old term suggested a crisis where none existed. Patients with severe elevations in BP but without signs of acute injury to brain, heart, kidneys, or eyes are not emergencies in the same sense. They do not require rapid BP lowering or parenteral drug therapy. Instead, for these patients the recommended approach is to reinstitute or intensify oral therapy, preferably managed in the outpatient setting with close follow-up.
A 2023 NephJC discussion tackled this very issue in the context of Inpatient Hypertension. The key message was clear: many inpatient BP spikes reflect context rather than crisis – driven by pain, anxiety, medications, or disrupted routines – yet they often prompt reflexive IV antihypertensive use. The parallel with “hypertensive urgency” is striking: numbers alone shouldn’t dictate emergency management. Instead, the emphasis should be on careful reassessment, addressing reversible contributors, and optimizing long-term therapy.
Table by Popa and Kurian, NephJC 2023
Consensus and Contrasts
The 2025 AHA/ACC hypertension guidelines arrived at a moment when global perspectives on BP management are converging, but not identical.
In the ESC 2024 document, the new update emphasizes lower targets, risk-driven management, and more rigorous detection strategies (McEvoy et al, EHJ 2024)
The International Society of Hypertension guidelines from 2020 (largely modeled on the 2018 ESH guidelines) aim to have a pragmatic focus for diverse health systems (Unger et al, Hypertension 2020)
The less said about the 2024 ESH guidelines the better - they are endorsed by the ERA, and have beta-blockers among first line agents (Kreutz et al, EJIM 2024).
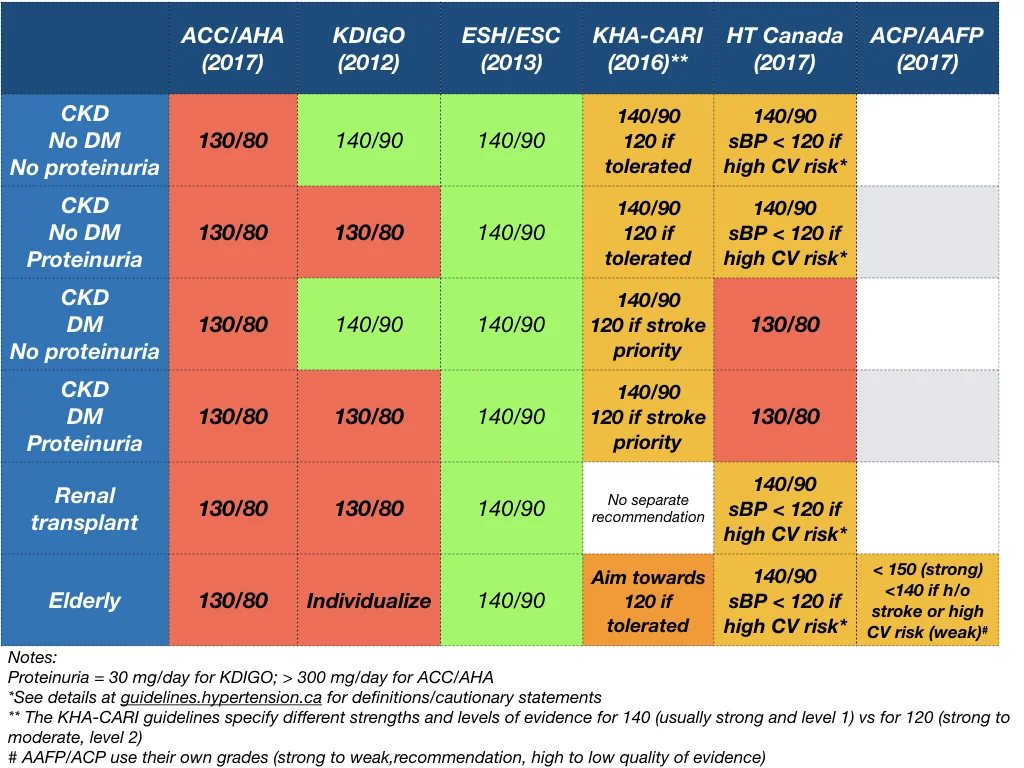
The KDIGO BP guidelines value cardiovascular prevention, and the SPRINT trial, and push for SBP < 120 in almost all CKD for that reason, with standardized BP measurement (KDIGO workgroup, Kidney Int 2021 | NephJC Summary).
Despite these differences in emphasis, the broad direction (except for ESH/ISH) is consistent: hypertension care is moving beyond the cuff to a more integrated, risk-oriented model. Areas of consensus are easy to spot – most notably, the reaffirmation of standard BP categories, recognition that CKD and albuminuria must be part of risk assessment, and the universal call for out-of-office confirmation of diagnosis.


Conclusion
The AHA/ACC 2025 hypertension guidelines sit alongside the ESC/ESH 2024, ISH, and KDIGO as part of a broader global conversation. While their approaches differ – be it risk calculators, pragmatic algorithms, or kidney-centered staging – the core principles align: screen carefully, stratify by risk, account for kidney health, and individualize therapy. For nephrology, the wins are undeniable: albuminuria testing is mainstream, CKD visibility is heightened, and aldosterone is on the radar.
Summary prepared by
Marc Lawrence Soco
Consultant Nephrologist
Chong Hua Hospital, Cebu, Philippines
Clemens Weber
Resident Internal Medicine
University Hospital, Mainz, Germany
Reviewed by
Cristina Popa, Pallavi Prasad, Brian Rifkin,
Swapnil Hiremath, Sayali Thakare
Header image created by AI prompts from Brian Rifkin