

With a healthy bump in participants post #ERAEDTA15, just compare the participants. 'Nuff said.
The American chat
The GMT chat

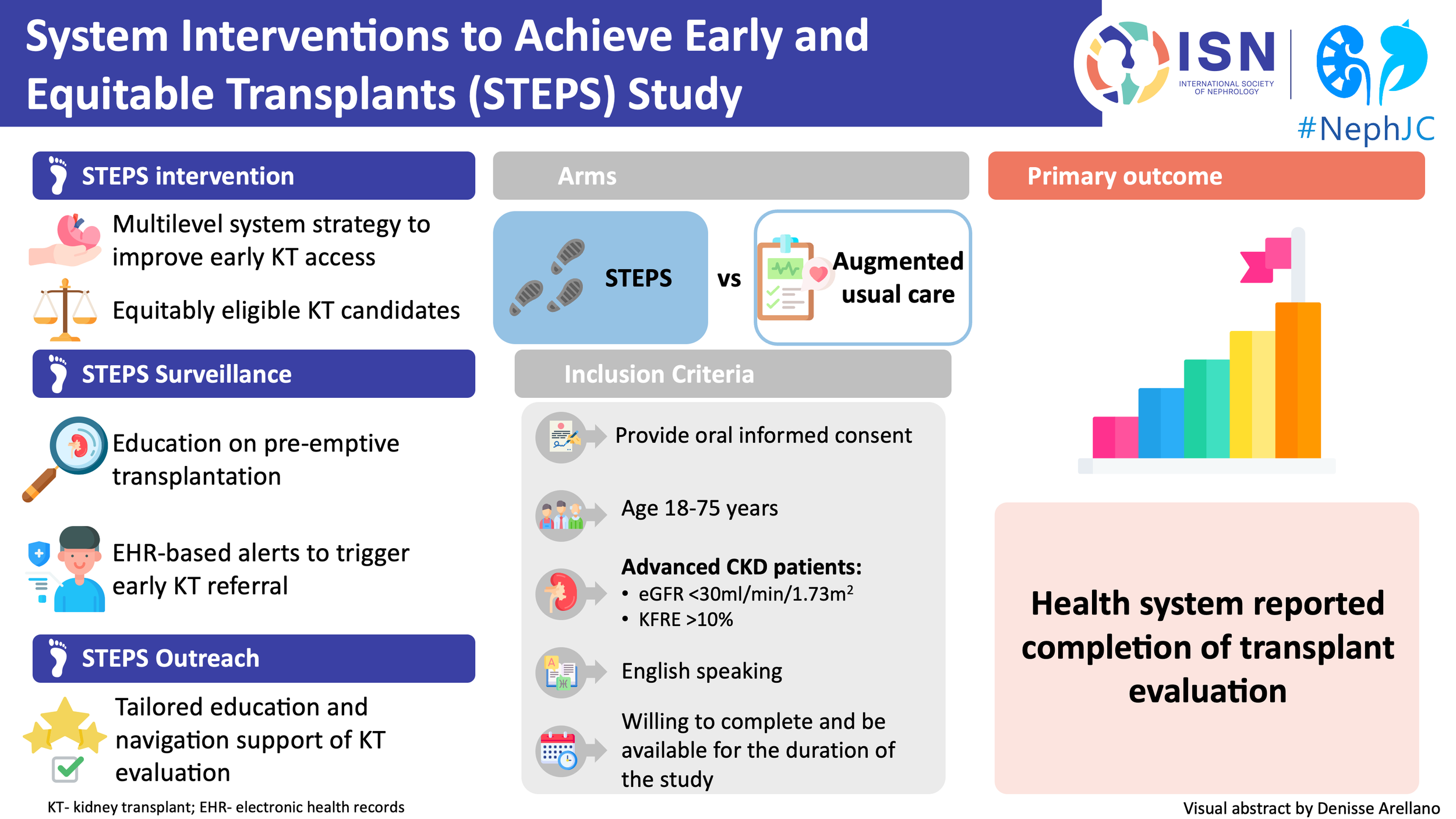
Summary of the STEPS trial which will be a twitter spaces discussion
This week, we will discuss the HIT trial- a large randomized study challenging one of the most reflexive responses in hospital medicine: see hyponatremia, fix the sodium. But what if correcting the number doesn’t change what actually matters?
This week, we will discuss the use of renal autologous cell therapy (REACT) in diabetic kidney disease.
With a healthy bump in participants post #ERAEDTA15, just compare the participants. 'Nuff said.
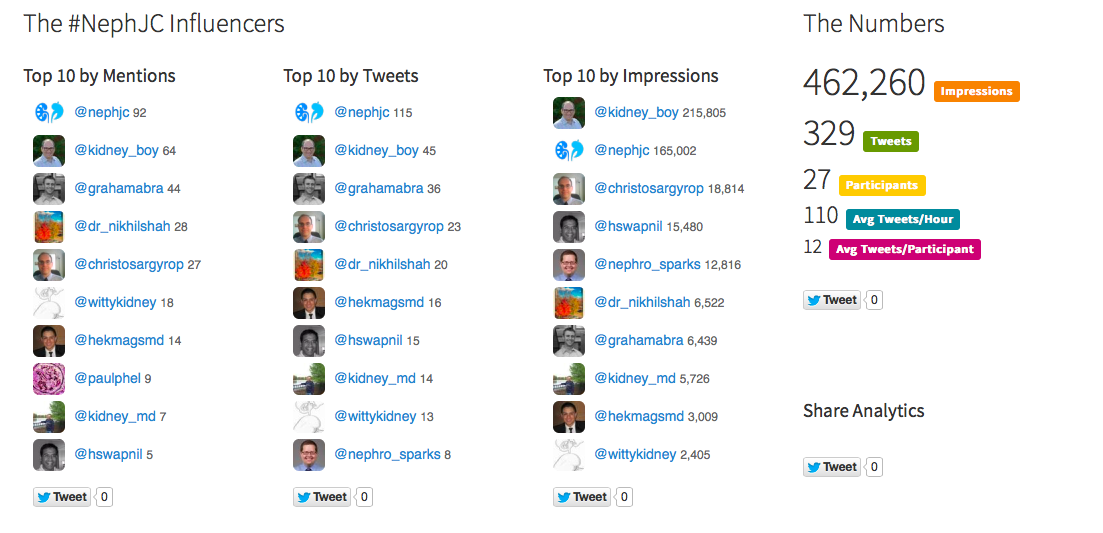
The American chat
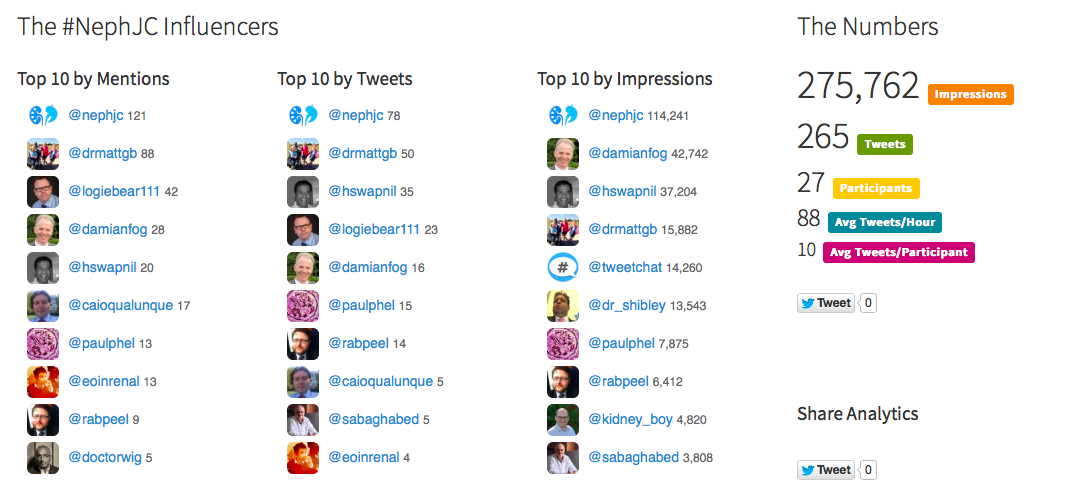
The GMT chat
As promised, the GMT chat storify is here, complete with the after party discussion on diuretics. Another superb curation by Hector!
Hector Madariaga - Nephrology Fellow from Syracuse and #NSMC intern - has now joined the #NephJC team. And you can see that why with the excellent job he has done with the storify of last week's chat. Watch this space for more contributions.
In case you were all wondering where the EU/African leg of the PD/CHF #NephJC chat disappeared, it will be held - albeit with a week's delay - on Wednesday June 3rd. It is all for a good reason. It has been quite busy for the Europeans this week - as you must have seen with all the furious tweeting from Charlie Tomson, Daniel McGuinness, David Arroyo, and many more including our very own Paul Phelan (who also wrote some excellent AJKD blog posts).

But, better late than never - and we hope many of you join us this week for the PD/CHF #nephjc chat.

Add this to the two articles by Alex Djuricich to flesh out your live-tweeting medical library.
The author and a number of AKI scientists joined NephJC Tuesday night to discuss F. Perry Wilson's study.


You may have seen the evidence pyramid before, with animal studies and case reports at the bottom, and systematic reviews on the top.

Well, an interesting paper was published a few days ago, in the Journal of Medical Internet Research. Go ahead, click on that link and check it out.
It is a systematic review of all twitter-based journal clubs (and they seem to have captured all that were existing at that time). They have then examined the impact of these journals clubs using many different metrics. Interestingly, the one that immediately stands out is in table 2:

Table 2 from Roberts et al, http://www.jmir.org/2015/4/e103/
There's only one journal club with over a million impressions. Take a bow, all of you who have ever participated in a #NephJC chat!
The paper does make for interesting reading, apart from what we mention above. Some of the analyses agrees with our thoughts after the first dozen #nephJC chats.
The chat begins at 9PM EDT, in just an hour. The topics will be:
From the ASN Advocacy and Public Policy page:

click the image to down load the 21 page house version of the bill.
If it wasn't from the pages of the New York Times I wouldn't believe it.

Please join us on #NephJC, Tuesday at 9PM EDT and Wednesday at 8PM GMT for a discussion of proper medical director behavior.
It was pretty well attended...

So was the GMT chat next day...

So our NSMC intern, Nikhil Shah not only did a super job of writing the sumary up for the BK virus #NephJC 22, he also has done a great job of curating the first chat into a storify.
The American chat (mostly by virtue of its longevity) still has more participants and tweets, but the GMT (EU/African) chat makes up by being fun and entertaining. Tom Oates, Paul Phelan, Francesco and their merry band of tweeters make for delightful reading. Jungle Juice, scud missiles and more. See some highlights below
@NephJC I never do EKG before starting quinolone, but always ask the patient: how long is your QTc? ;) #nephjc
— Fra Ian (@caioqualunque) March 4, 2015@ThePeanutKidney @NephJC Ideally when we use the untested jungle juice (cido,leflun,IVIg) we should do it as part of a study #nephjc
— Paul Phelan (@paulphel) March 4, 2015@swissnephro like the term PyVan 😄 pic.twitter.com/uA3wegSi1E
— John Booth (@ThePeanutKidney) March 4, 2015@NephJC nephrology's equivalent of a Scud missile - probably effective but lots of collateral damage #nephJC
— John Booth (@ThePeanutKidney) March 4, 2015
March is Kidney awareness month and in honor of that, Pallimed, the Hospice and Palliative Care Blog is talking about intersection of nephrology and palliative care. They asked NephJC co-creator, Joel Topf to host their chat. This happens on Wednesday. Topf wrote the introduction:
Have you ever read a journal article and as soon as you finished the abstract you had this forbidding feeling that if the authors actually proved what they claimed to have discovered your medical life will never be the same?
This happened when I read, Functional Status of Elderly Adults before and after Initiation of Dialysis by Tamura et al. in 2009.
The study simply looked at mortality and functional status of nursing home residents who initiated dialysis. The cohort consisted of 3,704 Americans. The average age of this predominantly white (64%) female (60%) cohort was 74 years. The outcomes were horrifying:
While this study did not track patients who deferred dialysis it is hard to imagine they could do much worse. The view of dialysis as a way to improve functional status by clearing uremia leading to improved nutrition and other downstream benefits was revealed to be a false hope. Instead we have a treatment that appears to be too rough for frail, at-risk patients and left them significantly worse than they were before dialysis.
The discussion section of the article had a sentence that should be embroidered to every nephrologists white coat:
“...kidney failure may be a reflection of terminal multiorgan dysfunction rather than a primary cause of functional decline, and thus the initiation of dialysis may not rescue patients from an inevitable decline.”
As nephrologists we need to elevate conservative, non-dialytic, therapy to be a clear option for patients, one that should be discussed along with peritoneal dialysis and transplant. Conservative care should not merely be a last resort when all other options have been exhausted.
I hope you will join us as we discuss the intersection of nephrology and palliative care this Wednesday at #hpm chat.

You might remember Perry Wilson, the young dapper nephrologist from Yale who presented his trial on AKI alerts at NephJC live a few months ago. He was tweeting as @nephrolalia - and has now renamed and rebranded himself as @methodsmanmd, which is quite apt given his recent blog posts and succinct and snappy videos up at MedPage Today.
More notably, the data he presented at #NephJC live has been published today - with some great additional analyses, in the Lancet. We sure know how to pick winners - so the next time we come calling, pick up the phone!
Dr. Faubel nailed the best comment about NephroCheck by reminding us while we pick apart the particulars of NephroCheck that we have some other dragons to slay:
@hswapnil @Nephro_Sparks @dr_nikhilshah btw, nephrocheck and urine eos cost about the same. urine eos useless. this much better. #nephjc
— sarah faubel (@doc_faubel) February 18, 2015
And then Edgar slides in with the appropriate #NephPearl (How does he do that so fast?)
@NephJC @doc_faubel Why I DO NOT order URINE EOSINOPHILS anymore #Nephpearls #NephJC http://t.co/NH9PdFK7fc pic.twitter.com/cbneNsoZPl
— Edgar V. Lerma (@edgarvlermamd) February 18, 2015
Last night we were off to a rollicking start with a great #NephJC chat - in great part due to the participation of Azra, Jay and Sarah! Joel took no time - burning the candle at both ends to do some storifys.
Here is the entire unedited archive with all the tweets from both chats:
The GMT chat today was also very intense - Storify will follow shortly!
Symplur don't lie



NephJC number 20 had the second most tweets and the third most participants. Thanks everyone for participating.

Discussing biomarkers.
{kind=link}