
#NephJCTenPosts 9 pm EST 7/7/26
Low-Dose Rivaroxaban and Cardiovascular Events in Advanced Kidney Disease:
The TRACK Randomized Clinical Trial
PMID: 42240165
Introduction
The concept of cardiovascular nihilism in advanced kidney disease stems from a paradox: heart disease is the leading killer in end-stage kidney disease, yet standard cardiological interventions consistently fail. While statin therapy reduces events in the general population, the AURORA (Fellstrom BC et al, NEJM, 2007) and 4D (Wanner C et al, NEJM, 2005) trials proved that aggressively slashing cholesterol was associated with zero reduction in cardiovascular death or strokes on dialysis. Similarly, the ISCHEMIA-CKD trial shattered the belief that mechanical intervention could fix the pathophysiology, revealing that immediate invasive revascularization failed to lower death rates and instead triggered a four fold increase in strokes (Bangalore S et al, NEJM, 2019| NephJC summary). In the uremic milieu, traditional lipid-driven and macrovascular models of heart disease stop applying.
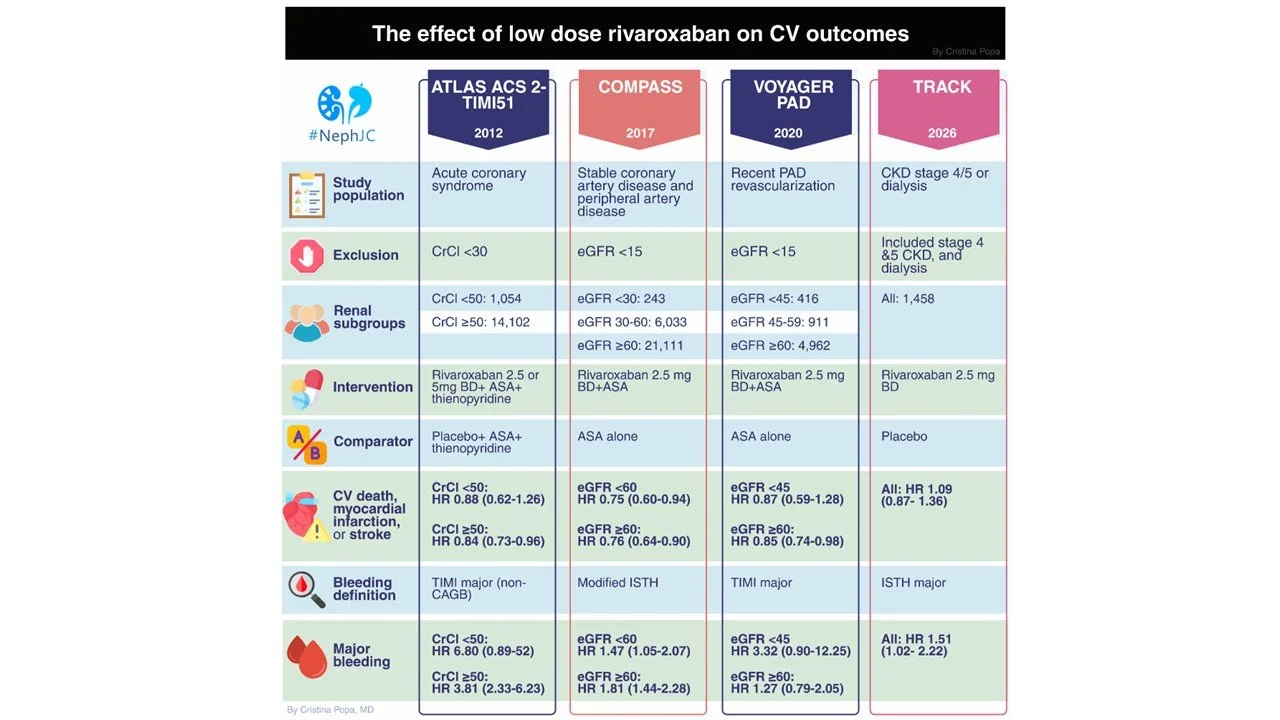
Driven by these failures, the scientific narrative shifted toward targeting hypercoagulability. Landmark trials in broader populations offered hope: COMPASS (Eikelboom JW et al, NEJM, 2017) demonstrated that adding low-dose rivaroxaban to aspirin significantly reduced major adverse cardiovascular events (MACE), with subanalyses hinting at greater benefits in mild-to moderate CKD (Fox KAA et al, JACC, 2019). This was reinforced by the VOYAGER PAD trial (Bonaca MP et al, NEJM, 2020), which proved that dual pathway inhibition decreased ischemic limb and cardiovascular events after peripheral revascularization, and the ATLAS TIMI ACS 51 trial, which showed a reduction in composite of cardiovascular death, myocardial infarction and stroke along with a significant reduction in risk of secondary outcome of stent thrombosis post-acute coronary syndrome (Mega JL et al, NEJM, 2012).
However, these practice-changing trials systematically excluded patients with stage 4 or 5 CKD and those on dialysis. Clinicians were caught in a dangerous blind spot: the KDIGO heat map definitively illustrates that as eGFR drops and albuminuria rises, CV risk skyrockets into the deepest red zone (KDIGO CKD guidelines 2024I NephJC Summary).
Yet, advanced kidney disease simultaneously induces severe platelet dysfunction and elevates the bleeding risk(Genovesi S et al, NDT, 2024). Doctors were forced to extrapolate data from healthier cohorts, flying blind without knowing if the ischemic protection seen in COMPASS, VOYAGER, and ATLAS would be wiped out by devastating hemorrhagic complications.
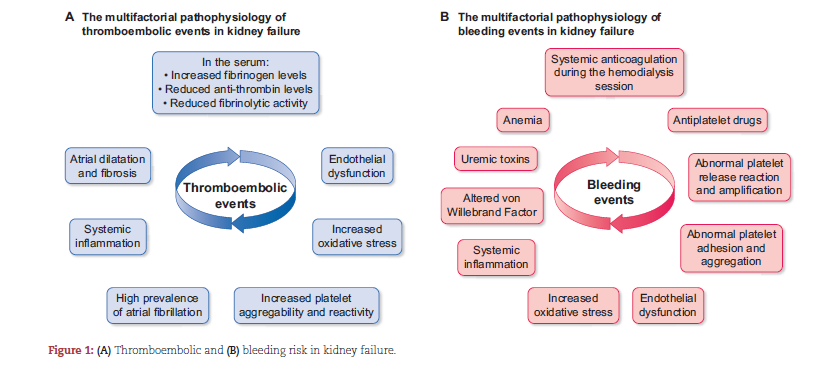
Figure 1 from Genovesi S et al, NDT, 2024
Figure 2 (supplement 1): 3- year incidence rate of major bleeding (per 1000 person years) by eGFR and ACR, from Badve SV et al, JAMA, 2026
The evidence gap justifies the need for the TRACK trial, which puts low-dose rivaroxaban to the test in patients with stage 4 or 5 CKD, including those on dialysis.
The Study
Study design
Investigator-initiated, randomized, quadruple-blind, placebo-controlled trial
Methods
The study was conducted at 90 centers in 12 countries (Australia, Belgium, Canada, France, Germany, India, Malaysia, Nepal, Saudi Arabia, Singapore, Taiwan, and Tunisia). The enrollment of patients was from January 18, 2021, to July 31, 2025. The trial was stopped early on August 7, 2025, based on the recommendation of the data and safety monitoring board, and final follow-up occurred on October 30, 2025.
Figure from supplement 1 (4.1): Schematic diagram of trial design, from Badve SV et al, JAMA, 2026
Funding
The major funding was provided by the National Health and Medical Research Council (NHMRC) Australia project grant, and additional funding was supplied by other participating centers. All funding was approved by the International Coordinating Centre for the George Institute of Global Health. Rivaroxaban and placebo tablets were provided by BayerAG free of cost through the Investigator-Initiated Research Support Scheme. The funders had no role in the design and conduct of the study, the data collection, management, analysis, or interpretation of the data, the preparation or review of the manuscript, or the decision to submit for publication.
Study population
Eligible participants were adults aged 18 or older with advanced CKD, defined as CKD stage 4 or 5, including those with dialysis-dependent kidney failure. All participants were required to have at least one additional cardiovascular risk factor, which could include established coronary artery disease, non-hemorrhagic non-lacunar stroke, peripheral artery disease, diabetes, or age 65 or older. Atrial fibrillation (AF) was not an inclusion criterion, but an exclusion criterion (see below).
Key exclusion criteria included mechanical/prosthetic heart valve, anticoagulation indication/contraindication, high bleeding risk or active bleeding, P2Y12 or phosphodiesterase inhibitor use, prior hemorrhagic/lacunar stroke, severe heart failure (EF < 30% or NYHA III/IV), hemoglobin < 90 g/L, thrombocytopenia, uncontrolled hypertension or a functioning kidney transplant. Patients with AF were excluded unless anticoagulation was not indicated.
Figure from supplement 1 of TRACK trial, from Badve SV et al, JAMA, 2026
Run-In Phase and Randomisation
Eligible patients were given a placebo for 21 days; the patients who were deemed to have < 80% adherence were excluded from the study (NephTrials on run-in periods for more). Randomization was performed through a web-based password-protected system, using a covariate-balancing adaptive allocation algorithm. The algorithm was designed to minimize between-group imbalances across four pre-specified stratification variables: diabetes, CKD stage, dialysis-dependency and aspirin use. Participants were allocated in a 1:1 ratio to receive either rivaroxaban 2.5 mg twice a day or matching placebo. All participants, investigators, study coordinators, site pharmacists, treating physicians, and outcome assessors were blinded to treatment allocation throughout the trial.
Outcomes
The primary efficacy outcome was a MACE composite of cardiovascular death, nonfatal MI, nonfatal stroke, or nonfatal peripheral artery disease event. The outcome was assessed by two investigators who were blinded; one was an on-site investigator and another member of the independent clinical outcome review committee (CORC).
Secondary outcomes included all-cause mortality; individual components of the primary composite outcome; a composite of CV death, MI, or stroke; a composite of infarction, stroke, or peripheral artery disease event; and venous thromboembolism. All deaths were adjudicated similar to the primary outcome.
The net clinical benefit outcome, initially classified as a secondary outcome, (later converted to a non secondary outcome before data review) was defined as a composite of CV death,nonfatal MI,non fatal stroke, a nonfatal peripheral artery disease event, fatal bleeding, or symptomatic bleeding into a critical area or organ.
Tertiary outcomes were thrombosis of dialysis vascular access among participants with AVF or AV graft and health-related quality of life (QOL) using EuroQ-5D-5L and cost-effectiveness. Cost effectiveness and EQ5D-5L were reported after getting complete data.
Safety outcomes were major bleeding (modified iSTH criteria: fatal bleeding, critical organ bleeding, bleeding requiring reoperation, or bleeding leading to hospitalization) and gastrointestinal bleeding. All bleeding was adjudicated by the CORC.
Additional data: Race and ethnicity were collected from the participants, as Asians are more prone to bleeding (Liang Y et al, JACC Asia 2024) and other comorbidity data were collected from medical records.
Statistical considerations
This trial planned to enroll 1900 participants over 3 years, with a follow-up period of 5 years. Assuming a control group primary event rate of 10 per 100 person-years, this sample size would provide a 90% power to detect a 25% relative risk reduction (hazard ratio 0.75) with a two-sided type I error rate of 5%. It was planned to conduct two equally spaced interim analyses with Haybittle-Peto efficacy boundaries, corresponding to a Z value of 3 standard deviations at each interim analysis. This yielded two-sided significance levels of 0.27% for each interim analysis and a final significance level of 4.82%. A total of 515 primary outcome events were required to achieve 90% power, and this number of events provided 80% power with a 22% relative risk reduction (HR 0.78).
All analyses were conducted according to the intention-to-treat principle. The primary outcome was analyzed as the time from randomization to the first event using a shared frailty Cox proportional hazard model with a random site effect, adjusted for the three stratification variables: 1) baseline aspirin use, 2) dialysis dependency and 3) diabetes. The final significance level was set at a 2-sided alpha of 4.86%, accounting for 1 interim analysis performed after 181 events.
The secondary outcome was also analyzed using the same Cox model. To control the family-wise error rate at 5% across the five key secondary outcomes—all-cause death and the four individual components of the primary composite—a Holm-Šídák step-down approach was applied. For the remaining secondary outcomes, no formal hypothesis testing was performed; only point estimates and 95% confidence intervals were reported. The proportion of adverse events, such as bleeding and severe adverse events, was analyzed using the Fisher exact test.
Results
Of 5,979 prescreened patients, 1,777 met initial eligibility criteria. After the run-in phase, 1,463 patients were randomized. Median follow-up was 1.7 years, with 93% completing the follow-up assessment. Loss to follow-up was minimal and similar in both groups (4% lost contact, 2.3% withdrew consent).
Figure 1. Flowchart of the trial, from Badve S et al, JAMA, 2026
The enrolled cohort was predominantly male (70%), had a mean age of 63 years, and nearly half (49%) had dialysis-dependent kidney failure. Most patients had diabetes (78%) and almost half (47%) were aged >65 years. Only 18% had established coronary artery disease and 6.6% had peripheral artery disease. Roughly two-thirds of the cohort met inclusion criteria based solely on diabetes or age, rather than prior CV disease. Aspirin use was identical between the arms (approximately 46%). Geographic representation was heavily concentrated in India and Malaysia (41.5% and 21%, respectively) (eTable 3 from Badve S et al, JAMA 2026)
Table 1. Baseline characteristics, from Badve S et al, JAMA, 2026
The trial was stopped early (Aug 2025), after 254 primary outcome events had occurred (49.3% of the 515 anticipated events). The Data and Safety Board recommended termination due to concerns about net harm.
Primary outcome
The primary composite outcome occurred in 164 patients (23%) receiving rivaroxaban vs 151 (21%) receiving placebo. This translated to 13 vs 11.8 events per 100 person-years, with a hazard ratio of 1.09 (95% CI 0.87-1.36). Rivaroxaban showed no benefit.
Figure 2. Cumulative incidence of the primary outcome, from Badve S et al, JAMA, 2026
Subgroup analyses confirmed uniformity of the null effect. Across age, sex, country, aspirin use, diabetes, CKD stage, and smoking history, no subgroups showed benefit. Aspirin use at baseline did not modify the treatment effect (HR 1.06 among aspirin users vs 1.11 among non-users).
eFigure 4: Subgroup analyses, from Badve et al JAMA 2026
Mortality
All-cause mortality showed no difference. In the rivaroxaban group, 25.6% died compared with 23% in placebo- 13.9 versus 12.4 events per 100 person-years (HR 1.14, 95% CI, 0.92-1.40). There were 18 more deaths in the rivaroxaban group overall.
The competing risk analysis examined whether the high non-cardiovascular death burden distorted the primary outcome estimate. Accounting for the non-cardiovascular death as a competing event yielded a subdistribution HR of 1.08 (95% CI 9.86-1.34) for the primary outcome. As regards the cumulative mortality (eFigure 1) at 48 months, the rivaroxaban curve remained above placebo (51% vs 47%)
eFigure 2. Primary outcome by competing risk analysis, from Badve S et al, JAMA, 2026
The breakdown of mortality causes (eTable 4 below) showed that 60% were cardiovascular deaths in the rivaroxaban arm. Sudden cardiac death, occurring outside the 30-day window after acute MI, dominated both groups (40% in the rivaroxaban arm vs 45% in the placebo arm). Infections were the leading non-CV cause, followed by renal failure and other organ-system failures.
eTable 4. Causes of death, from Badve S et al, JAMA, 2026
Secondary outcomes
Individual components of the primary outcome were comparable between the two arms. Additionally, when the events were recombined into secondary composite endpoints, rivaroxaban showed no advantage across any configuration (Table 2 below).
able 2. Efficacy outcomes, from Badve S et al, JAMA, 2026
Venous thromboembolism
Fewer VTE events occurred on rivaroxaban than on placebo (0.6% vs 1.9%), with aHR 0.29, 95%CI 0.09-0.87.
Among patients on hemodialysis, access thrombosis occurred more frequently on rivaroxaban (7.6% vs 5.4%), but the result was not significant (HR 1.44, 95% CI, 0.75-2.74).
Safety outcomes: major bleedings
Major bleeding events occurred more in the rivaroxaban group (8.8% vs 6%), with a HR of 1.51 (95% CI 1.02-2.22).
Table 3. Bleeding events and net clinical benefit outcomes, from Badve S et al, JAMA, 2026
The sites and characteristics of major bleeding are detailed in eTable5 (below). The gastrointestinal tract was the most common site. These events included overt bleeding confirmed by endoscopy, overt bleeding of unknown origin, and presumed occult bleeding with hemoglobin decrease.
eTable 5. Bleeding events, from Badve S et al, JAMA, 2026
Intracranial and intraocular bleeding were numerically higher in the rivaroxaban group. Fatal bleeding occurred in 1 patient on rivaroxaban and 2 patients in the placebo group.
Bleeding by age
Major bleeding risk showed significant age interaction (eFigure 5 below). In patients ≥65 years, major bleeding occurred in 10% on rivaroxaban vs 5.6% on placebo. In those <65 years, the rates were lower (rivaroxaban 7.3% vs 6.4% in placebo) and comparable.
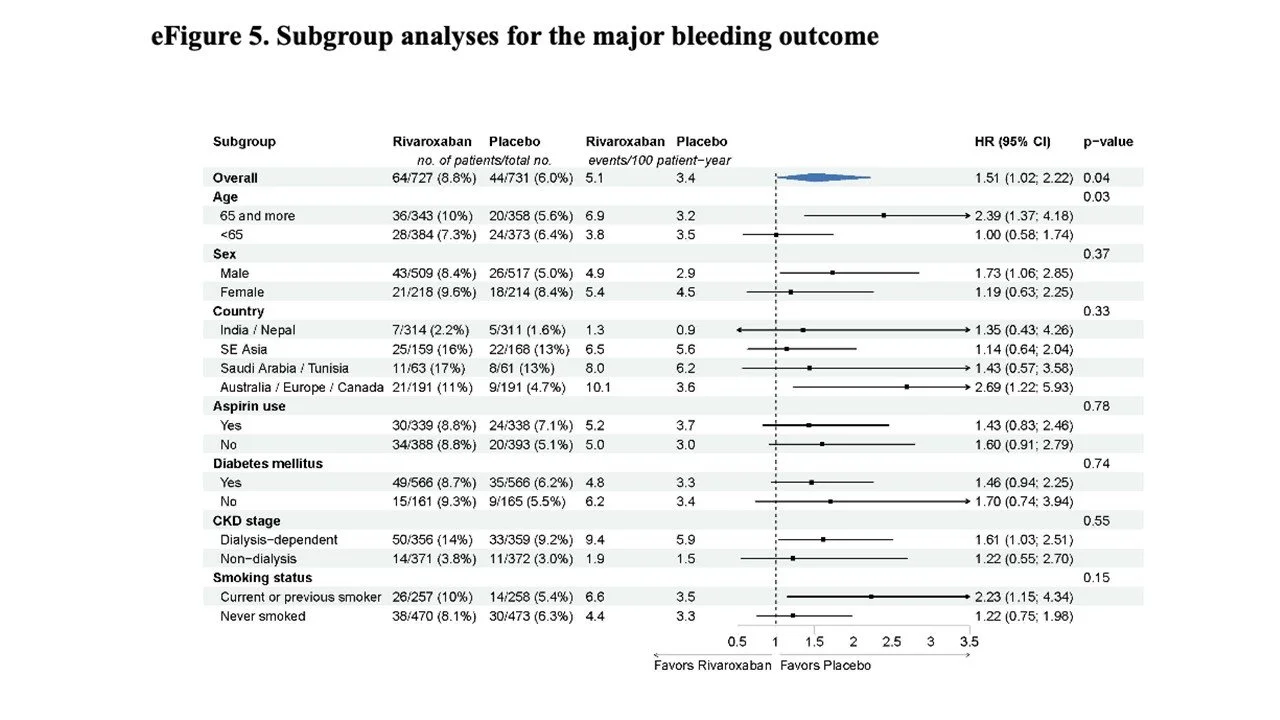
eFigure 5. Subgroup analyses for the major bleeding outcome, from Badve S et al, JAMA, 2026
Net clinical benefit
The net clinical benefit outcome (composite of cardiovascular events and fatal/critical bleeding events) was comparable between the two arms (24.2% rivaroxaban vs 21.3% placebo, HR 1.14, 95% CI 0.92-1.41- details in Table 3 above)
Serious adverse events
They were similar between the groups. Infections were the most common (17.6% rivaroxaban vs 18.1% placebo). Overall, 50.5% of rivaroxaban patients and 45.8% of placebo patients experienced ≥ 1 serious adverse event.
Discussion
TRACK randomized more than 1400 patients with CKD stage 4, 5 or dialysis-dependent kidney failure, enriched for CAD, prior stroke, PAD, diabetes, or age 65 and older, to rivaroxaban 2.5 mg daily or placebo. The question was whether the “vascular dose” anticoagulation in COMPASS (Eikelboom JW et al, NEJM, 2017) and VOYAGER PAD (Bonaca MP et al, NEJM, 2020) would be of benefit to a population with advanced CKDs, and… it wasn’t. The primary MACE composite (CV death, MI, stroke, and PAD event) was not significantly different in rivaroxaban vs placebo (22.6% vs 20.7%). What’s even worse, major bleeding was higher on rivaroxaban, so this was not a benign intervention. The DSMB stopped the trial early after a post hoc conditional-power calculation put the chance of eventual benefit at 16% with a HR of 0.78 even if the trial continued till the pre-specified 515 primary events. Net clinical benefit, the composite meant to weigh efficacy against safety, was also negative. The study excluded patients with a clear indication for anticoagulation; rather, it tested whether across the board anticoagulation was worthwhile in high-risk CKD patients whose vasculature has already been modified by uremia.
Context
The vascular-dose approach isn’t new. ATLAS TIMI 51 (Mega JL et al, NEJM, 2012) identified 2.5 mg twice daily as the dose that balanced antithrombotic benefit against bleeding, and a pooled analysis of seven trials across over 45,000 patients with CAD or PAD found low-dose rivaroxaban added to antiplatelet therapy reduced CV events (HR 0.86, 95% CI 0.78-0.94) and ischemic stroke (Bucci T et al, J Clin Med, 2024). Trials like COMPASS (Eikelboom JW et al, NEJM, 2017) and VOYAGER PAD (Bonaca MP et al, NEJM, 2020) enrolled patients with established atherosclerotic disease. TRACK’s population looked different: only ~19% had coronary disease, ~ 6% had prior stroke, ~6% had PAD, and 57% qualified on the strength of a single risk factor, usually age or diabetes alone (eTable 3). Either way, this looks closer to a primary-prevention population that the trials TRACK was built to extend, and it points to a precedent worth naming directly: aspirin’s own run of primary-prevention trials a decade earlier. Three trials tested low-dose aspirin for primary cardiovascular prevention in similarly enriched, disease-free populations. ASCEND, in adults with diabetes and no prior cardiovascular disease, found a 12% relative reduction in vascular events “largely counterbalanced” by a 29% increase in major bleeding, in the authors’ own phrasing (The ASCEND Study Collaborative Group, NEJM, 2018). ASPREE, in adults 70 and older without prior cardiovascular disease, found daily aspirin gave no cardiovascular benefit and significantly increased major hemorrhage (McNeil JJ et al, NEJM, 2018). ARRIVE, in moderate-risk adults without diabetes, found that aspirin had neither benefit nor safety (Gaziano JM et al, Lancet, 2018). None of these 3 trials used rivaroxaban or any other DOAC. But TRACK’s age and diabetes-heavy cohort sit roughly in the territory they mapped, and a different antithrombotic drug, tested there again, produced the same shape of result: no measurable protection and hemorrhagic side effects.
Guidelines
KDIGO’s 2024 CKD guideline draws a sharp line between two questions it treats differently. (KDIGO CKD Work group, Kidney Int, 2024| NephJC summary). For secondary prevention- aspirin in people with established CVD- it gives a strong graded recommendation (1C), built on Antithrombotic Trialists’ Collaboration meta-analysis: a roughly 19% relative reduction in serious vascular events (RR 0.82, 95% CI 0.75-0.87) (ATT collaboration, Lancet, 2009). For primary prevention, aspirin in people at high risk without established disease (the category TRACK mostly falls into), KDIGO issues no graded recommendation at all, only a call for more research. Its reasoning was that ASCEND, ASPREE, and ARRIVE all showed bleeding harm counterbalancing aspirin’s CV benefit. A CKD-specific Cochrane meta-analysis of more than 40,000 participants in antiplatelet versus placebo trials found similar results: MI reduced (RR 0.88, 95% CI 0.79-0.99), major bleeding increased (RR 1.35, 95% CI 1.10-1.65)- though that analysis didn’t separate primary from secondary prevention (Natale P et al, Cochrane Database Sys Rev, 2022)
The answer is “No”
Advanced CKD is often described as a state where clotting and bleeding risk rise together. The mechanism implies uremic toxins impair platelet adhesion and drive endothelial nitric oxide and prostacyclin production that further suppresses clotting, leaving CKD patients roughly 1.5 times more likely to bleed than people with normal kidney function, independent of antithrombotic use (Ocak G et al, J Thromb Haemost, 2018). Hemodialysis adds a further 1.5-fold risk over peritoneal dialysis (van Eck van der Sluijs A et al, NDT, 2021), and roughly one in seven older patients on dialysis has a major bleed within 3 years of initiation (Sood MM et al, Kidney Int, 2013). TRACK asked a fair question and got a clear answer. Rivaroxaban didn’t protect against clots, and it increased bleeding~ extra 1.7 events per 100 patients-years(Table 3). The only positive, VTE (HR 0.29), is more a pharmacological note- with what clinical significance? The bleeding risk fell hardest on patients 65 and older (interaction P = .03), the group most likely to get this drug in clinical practice.
On a less nihilistic view, a negative, well-done trial like TRACK is an answer. The mechanism was plausible, the drug worked in other settings, and the patients carried a real risk- reason enough to run the trial. The result, rigorously tested and honestly reported, is worth as much as a positive one: it tells clinicians where not to engage in speculative benefit when there is significant risk of harm. Aspirin’s primary prevention trials reached a similar answer a decade ago, in a different population, with a different drug. TRACK adds a boundary, drawn a second time in roughly the same place - here is where “thin the blood, protect the vessel" stops working.
Strengths
TRACK trial was a dedicated, investigator-initiated, randomized, double-blind, placebo-controlled trial across 90 centers in 12 countries, enrolling adults with CKD stage 4 or 5, including dialysis. Randomization was stratified and blinded at all relevant levels, with a covariate-adaptive algorithm balancing key prognostic factors. Prespecified outcomes were adjudicated by an independent clinical outcomes committee (essential when effects are modest and noise is abundant).
Limitations
The trial was powered for 1900 participants and 515 primary events, but it stopped early at 1463 randomized patients based on DSMB recommendation for futility (conditional power ~ 16% for HR 0.78), not a prespecified efficacy boundary. Follow-up was a median of 1.7 years, shorter than planned, and formal tablet counts were disrupted by COVID-19, though self-reported adherence was collected. Permanent discontinuation was 28%, which likely attenuated any true effect. The confidence interval for the primary outcome (0.87-1.36) rules out a large benefit but leaves modest effects uncertain.
About generalizability: there were no US patients and almost no Black patients. Regional variation was observed (Australia/Europe/Canada- for primary outcomes: HR 1.82, 95% CI 1.02-3.22), but interaction tests were not significant, and this was an unadjusted subgroup comparison, hypothesis-generating only. Nearly 40% of all-cause deaths in both arms were sudden cardiac death, a category that no anticoagulant was likely to prevent, which sets a biological ceiling on what this class could achieve. Minor bleeding was not collected, and quality-of-life data are deferred to a separate report. While 46% of patients were on aspirin at baseline, the trial did not mandate aspirin nor test the fixed combination- unlike COMPASS and VOYAGE PAD.
Conclusion
TRACK doesn’t solve advanced CKD’s oldest problem- a body where treating one risk worsens another, with no drug built for that narrow ground. It settles the case against rivaroxaban. Unfortunately, push clotting down, and bleeding rises to meet it: the scales of hypercoagulability and excessive bleeding are never completely balanced. The boulder keeps returning to the bottom by a different route, and no antithrombotic strategy tried so far has gone over the hill instead of around it. That may be the shape of the answer for this population: something closer to a limit than a solution, since one antithrombotic therapy alone was always going to run up against the complex CKD pathophysiology.
Summary by,
Reviewed by Brian Rifkin, Pallavi Prasad,Swapnil Hiremath