
Intro
The most fundamental advice for stone formers is simple: drink more.
How much? More. No matter how much urine you make, if you can make more you will do better, but more than 2.5 liters is the goal. We don’t actually care how much you drink—we care how much you pee. The goal is >2.5 liters of urine, because dilution fixes the chemistry that drives stones.
But patients don’t care about urine chemistries—they care about avoiding stones. And that’s where things get hard.
Stone trials with stone events are brutal. Events are slow, unpredictable, and unforgiving. They have a habit of wrecking dogma.
NOSTONE is the perfect example—thiazides improved urine chemistry and CT findings, but didn’t reduce patient facing stone events.
Now patient-centered outcomes come for the granddaddy of all advice: drink more water.
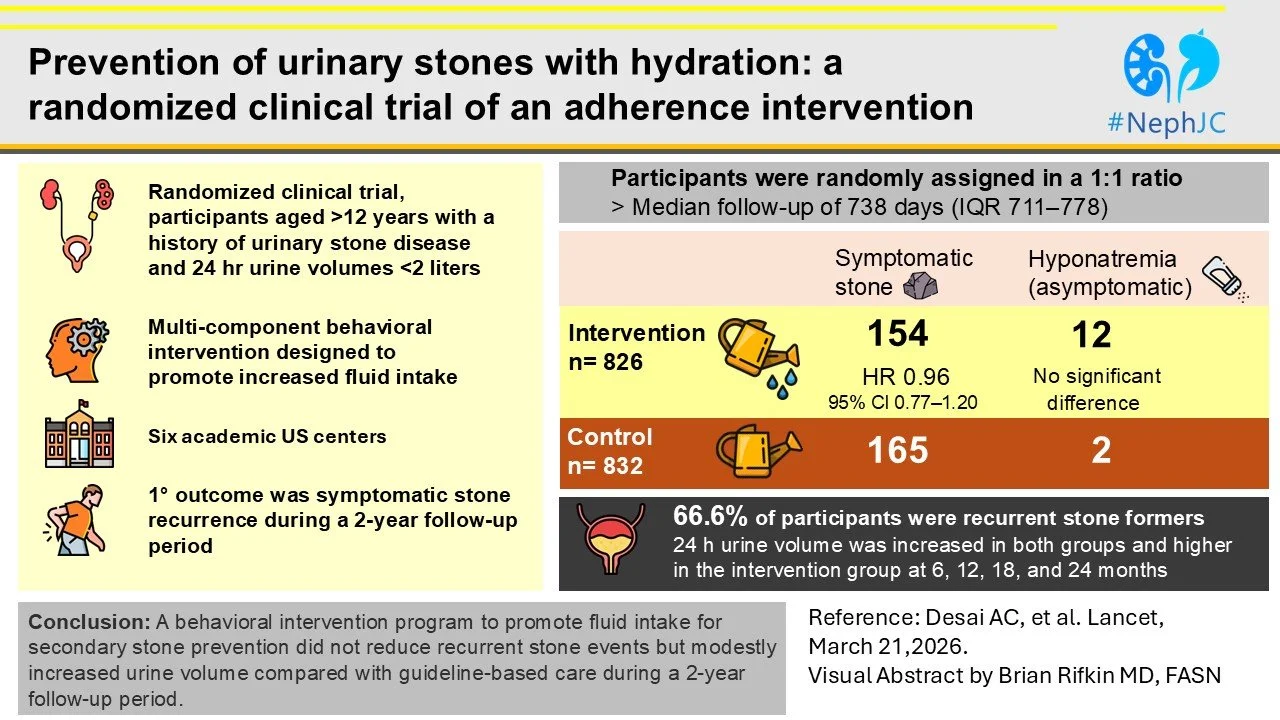
The PUSH trial (Lancet 2026) randomized patients to an aggressive, behaviorally engineered hydration strategy versus usual care (which, in stone disease, of course, is “MORE WATER”).
Once again, the RCT shows up and steals our favorite toy.
Let’s take a look at this trial before it is memory holed by every stone specialist.
Before we dive further into PUSH we should understand a bit of the prior art:
The most important study is an Italian RCT by Borghi, Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study (J Urol 1996) These guys enrolled patients, after their first kidney stone and randomized them to either:
Being told to drink a lot of water or
Being told, “Since it is your first kidney stone, there is no need to make changes to your diet.”
That’s it. That’s the intervention.
But the trialists must have been devastatingly persuasive.
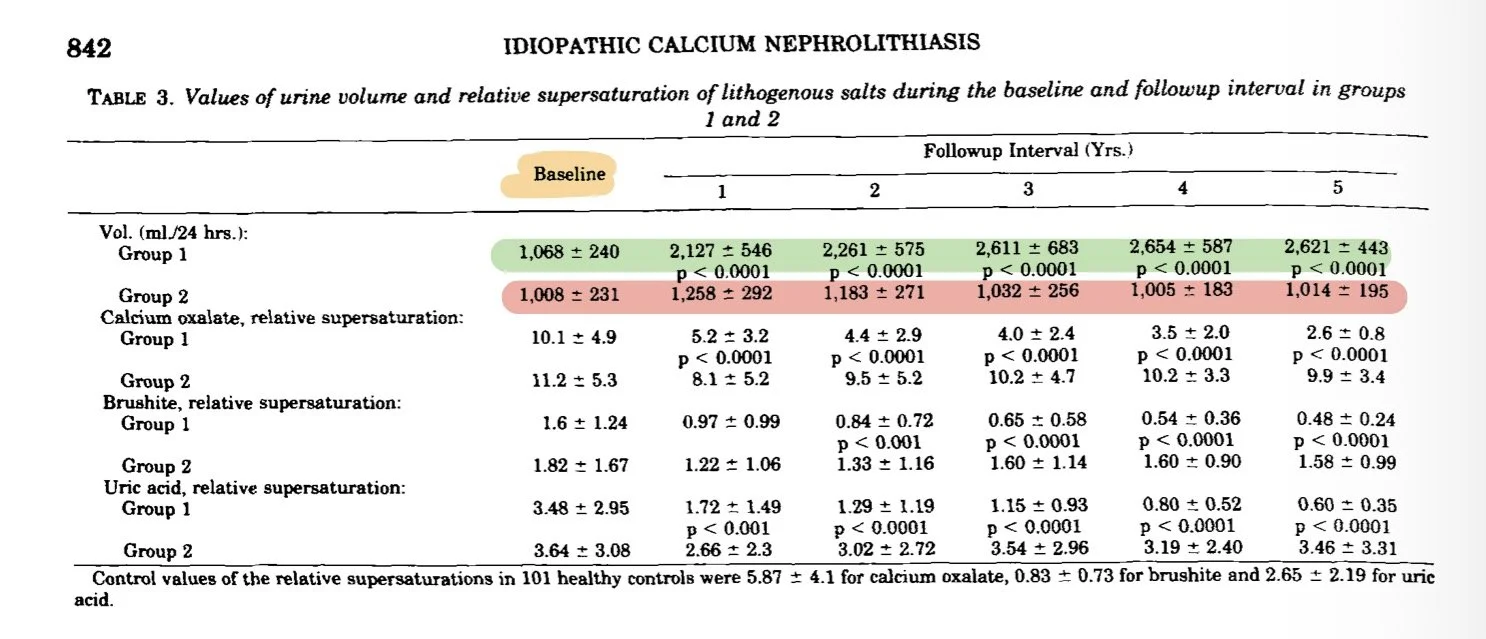
People told to drink a lot of water immediately doubled their urine output and over time further increased their urine output to 2.6x their baseline urine volume. Patients in the control group had a modest 20% increase in urine volume for the first year and then reverted back to their baseline urine volume for years 2-5.
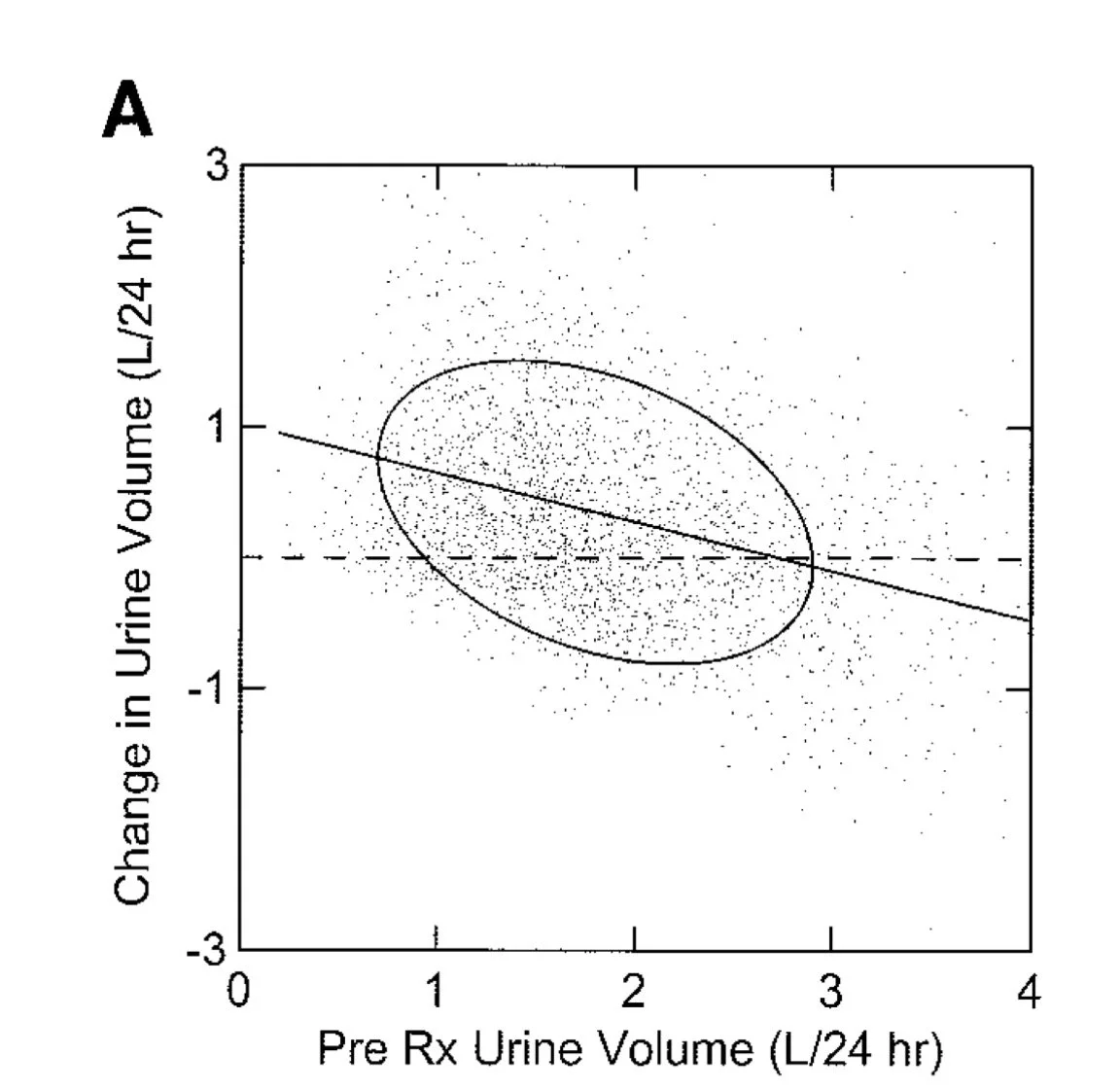
I hope I sound skeptical because I am. This sounds like bullshit to me. When Fred Coe (Changes in urine volume accomplished by physicians treating nephrolithiasis J Urol 2003) looked at how much urine volume increased following patients engaging a kidney stone doctor, he found a delta of 300 ml, not the 1600 ml the Italians “found.” Intrerestingly Coe found that the bump in urine volume was inversely proportional to the initial urine volume (reversion to mean or something else?).
Now back to PUSH
METHODS
Participants
The investigators targeted patients with a recent stone event (in the last 3-years, or in the last 5-years if there was also a new stone by U/S or CT).
Only patients with less than 2 liters of urine were randomized, exactly the patients we tell to drink more water. This setup raises a concern: regression to the mean could inflate urine improvements in both groups.
Intervention
Every nephrologist has their little advice they give people to get them to drink more and instagram has an entire cottage industry dedicated to convincing people to increase their water intake. PUSH didn’t just say “drink more”—it engineered behavior:
Loss framed payments for drinking water. People were promised $1.50 a day unless they drank less than 2.5 liters a day. Very Kahneman and Tversky. This stimulus was gradually reduced over time
Coaching with structured problem solving to get participants to DRINK MORE
Text reminders and social nudges
The control got the usual, “drink more water” pep talk!
Assessment
Intake was tracked with Bluetooth water bottles. Very 2020s
Stone events were investigated by a blinded adjudication committee. I love that patients qwere not trusted to adjudicate their own patient reported outcomes.
Secondary outcomes were exhaustive including serial CT scans and 24-hour urines.
Power analysis
The needed 821 group to reach 80% power to detect a 30% reduction in stone events at 2 years. Yikes, that is a large effect size. They assumed a 15% event rate with 20% attrition.
RESULTS
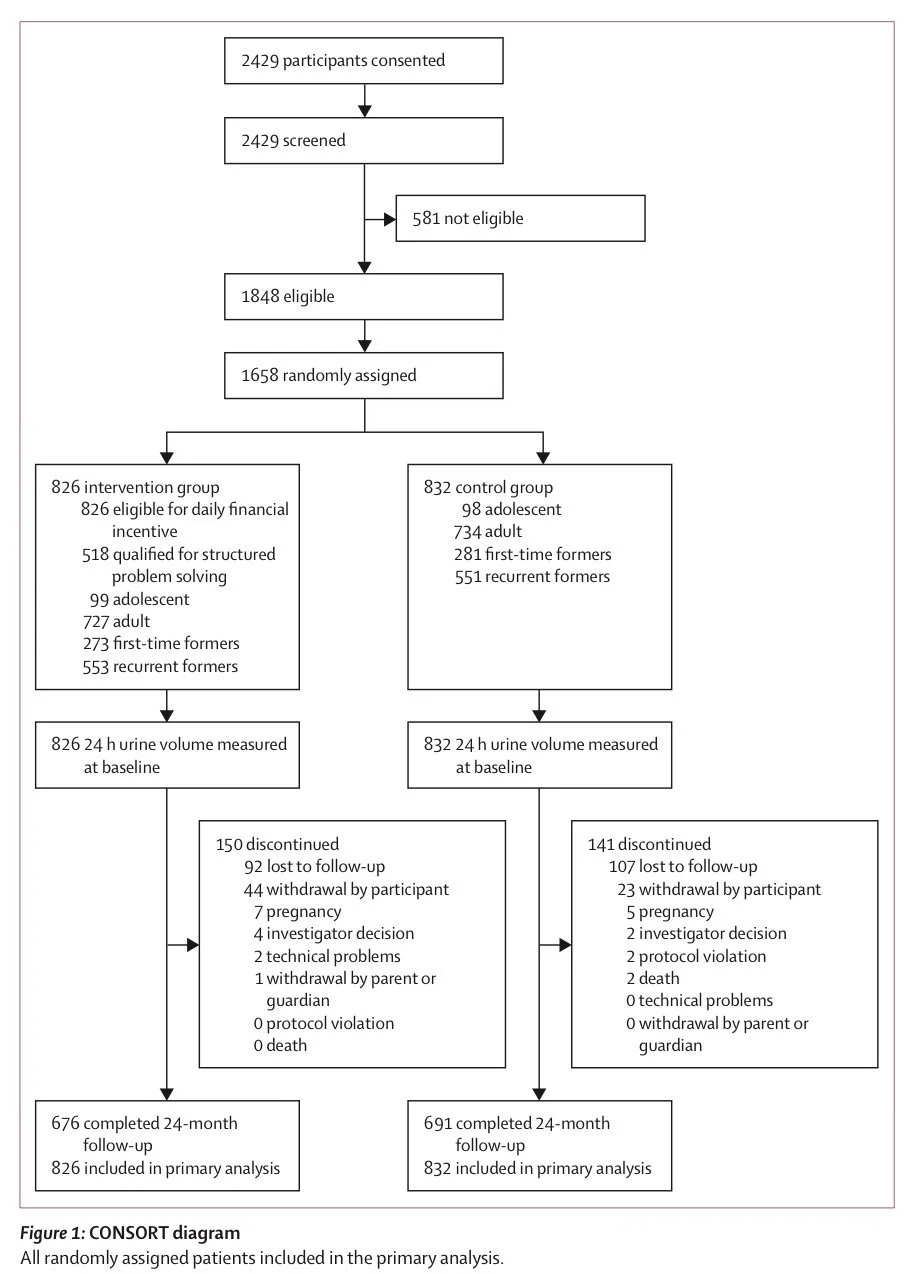
They nailed enrollment and retention, an under-appreciated win (1658 enrolled compared to 1642 estimated; 1367 retained, above the 1326 estimated).
Demographics
They had more women than men. We don’t see that often in studies. Maybe this was due to the requirement for low water intake for enrollment?
Baseline Urine
Baseline use of anti stone therapy was modest, 7% thiazide and 11% KCitrate.
Baseline urine chemistries were surprisingly normal. The standout abnormality was volume: 1.3 L/day.
Primary Outcome
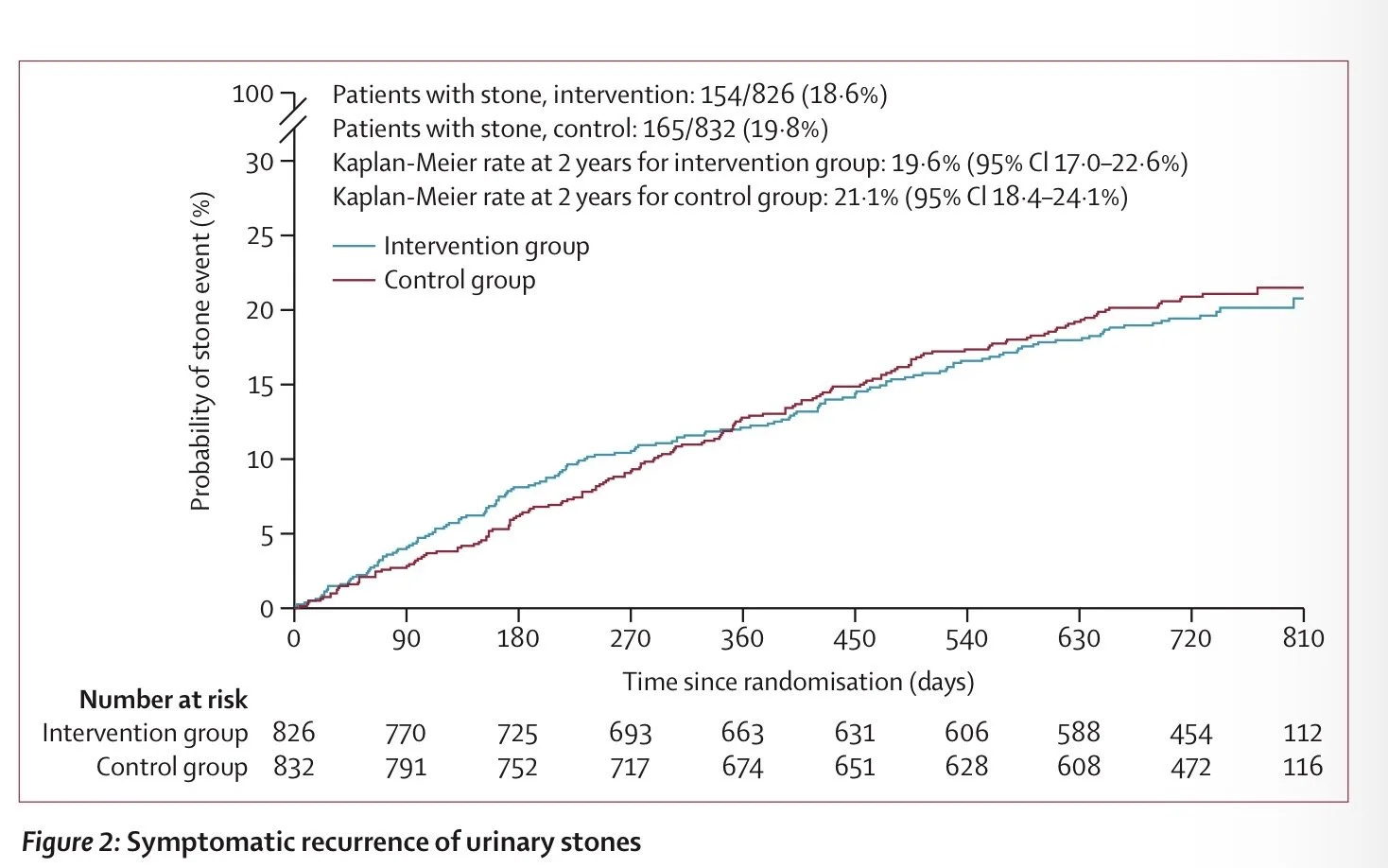
After 2 years 19% in the intervention group had a stone events compared to 20% in the control group. No signal.
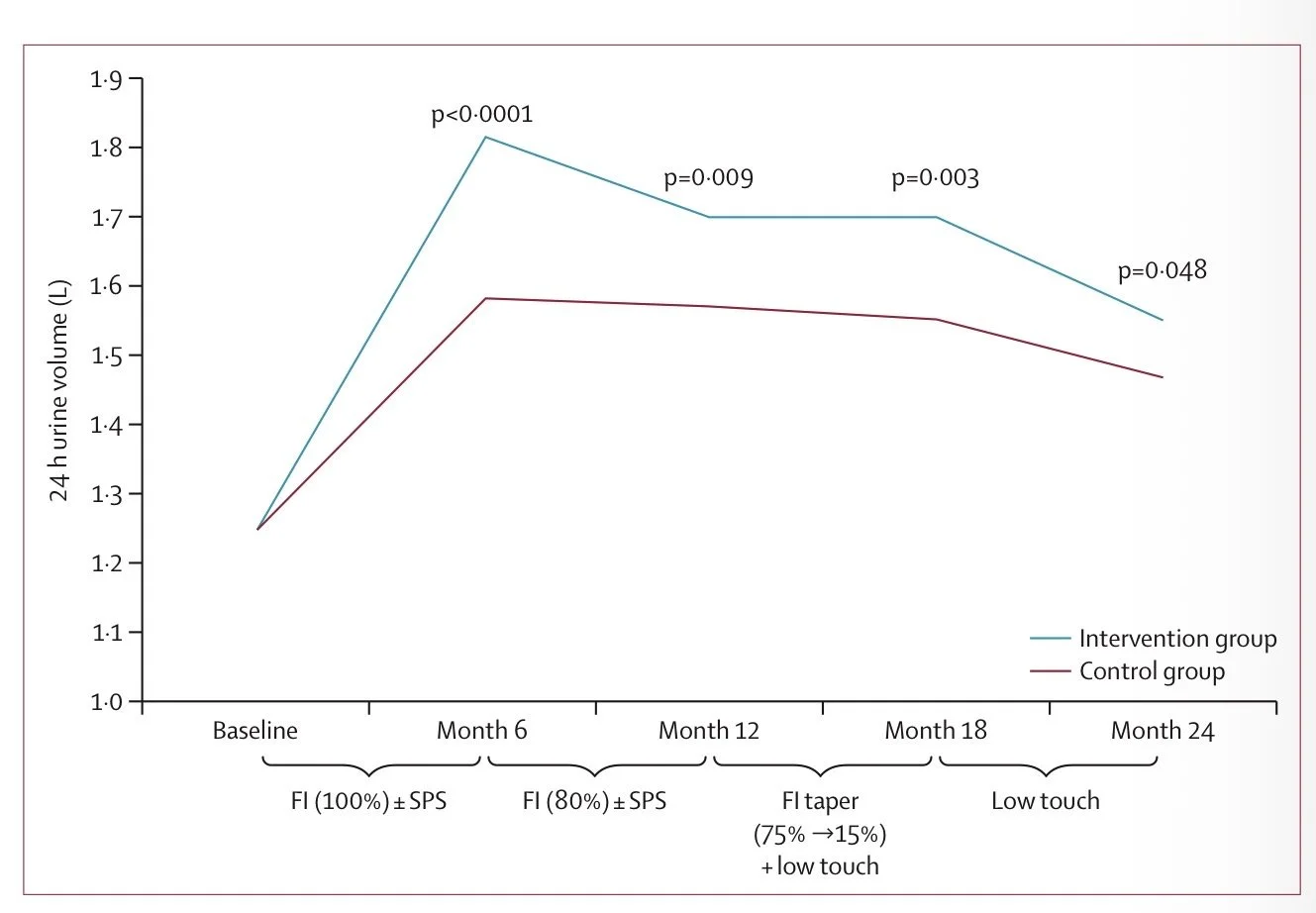
The intervention increased urine volume, but the effect faded over time and never reached the 2.5 liter target.
In the control group we have nice Hawthorne effect versus reversion to the mean.
The serial CT scans showed no difference in stone growth or reduction in the development of new stones.
Adverse effects
The intervention group drank ~28 extra gallons over 6 months.
And what was the payoff?
More urgency, more frequency, and more nocturia.
More water. More symptoms. No benefit.
The authors considered if the trial would have shown a different result if it went longer. They concluded, “The follow-up period was only 2 years; however, the PUSH trial exceeded the estimated event rate, and the Kaplan–Meier curves were nearly parallel, suggesting that a longer follow-up period for PUSH is unlikely to change the results.”
Conclusion
So what did PUSH actually show?
Not that water doesn’t work.
It showed that even an intensive, multi-layered, evidence-based behavioral intervention cannot increase hydration enough to prevent stones.
This is less a failure of physiology and more a failure of our ability to change behavior.
Ooof.
Kidney stones clinics take another one on the chin.