
#NephJC Chat
Tuesday May 26th, 2020 at 9 pm Eastern Daylight Time
Wednesday May 27th, 2020 at 9 pm Indian Standard Time
Wednesday May 27th, 2020 at 9 pm BST
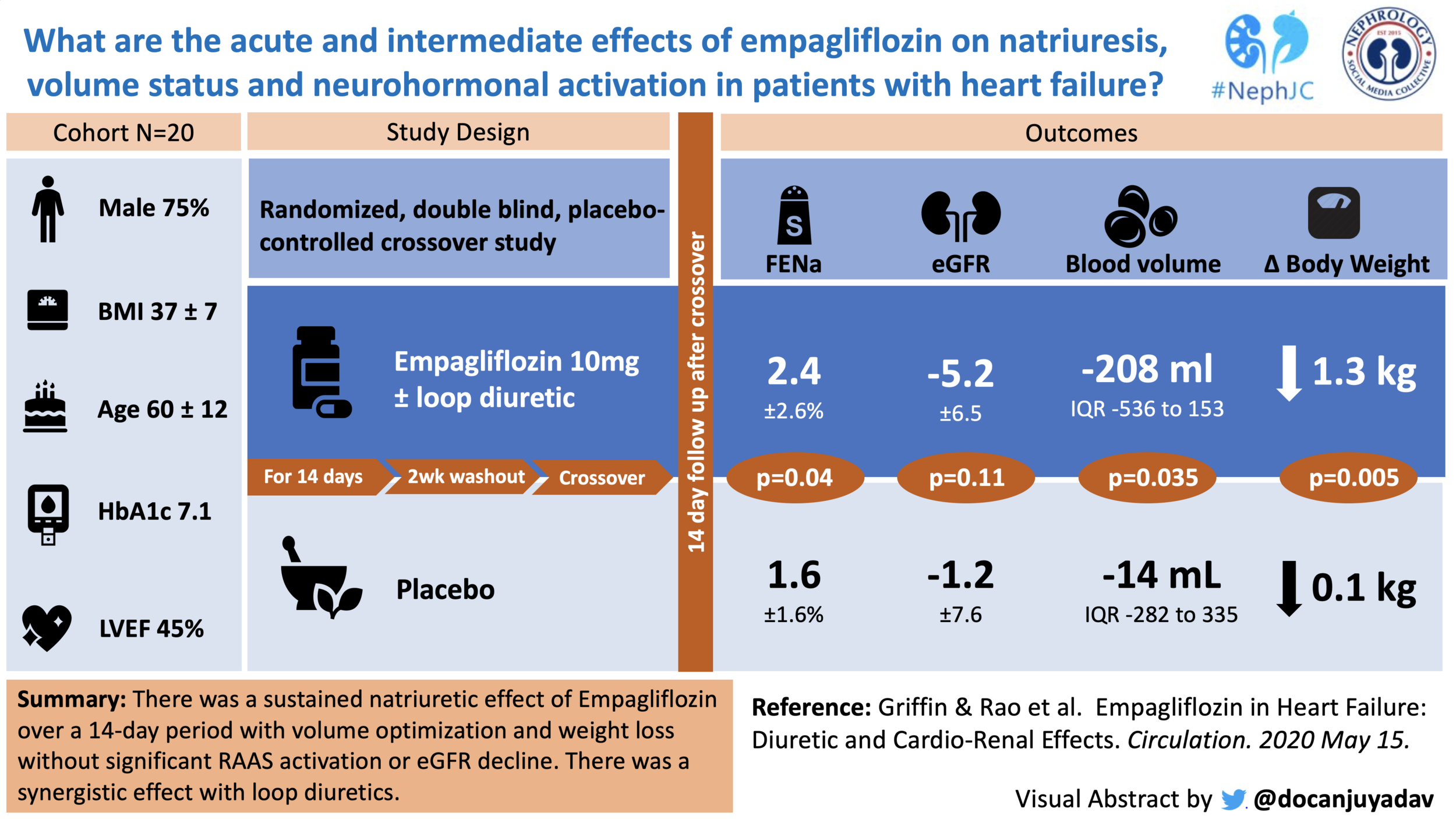
Empagliflozin in Heart Failure: Diuretic and Cardio-Renal Effects
Matthew Griffin, Veena S Rao, Juan Ivey-Miranda, James Fleming , Devin Mahoney, Christopher Maulion, Nisha Suda, Krishmita Siwakoti , Tariq Ahmad, Daniel Jacoby, Ralph Riello, Lavanya Bellumkonda, Zachary Cox, Sean Collins, Sangchoon Jeon, Jeffrey M Turner, F Perry Wilson, Javed Butler, Silvio E Inzucchi, Jeffrey M Testani
PMID: 32410463 Full Text at Circulation.


Introduction
SGLT2 inhibitors (SGLT2is) have emerged as a promising new therapy that lowers morbidity and mortality in diabetes by impeding cardiovascular disease (CANVAS, EMPA-REG, DECLARE-TIMI 58) and chronic kidney disease (CREDENCE). This class of medication lowers blood glucose by inhibiting the SGLT2 Na/glucose co-transporter in the proximal tubule (PT). With maximal dosing, reabsorption of filtered glucose is lowered from essentially 100% to around 30% (in the presence of SGLT2 blockade, SGLT1 increases resorption activity).
The role of SGLT2is in non-diabetic patients is among the hottest topics in medicine currently. ICYMI, it won the NephMadness 2020. The DAPA-HF trial showed that dapagliflozin halts heart failure progression and lowers cardiovascular mortality in patients with and without diabetes. An analogous study in kidney disease (DAPA-CKD) has been stopped early due to the “overwhelming efficacy [of dapagliflozin] in patients with CKD”.
Clearly, the benefits of SGLT2is extend beyond their role in glycemic control. But how? Two potential mechanisms were reviewed in this year’s NephMadness SGLT2i region: activation of tubuloglomerular feedback (TGF) and direct protection against pathologic podocyte remodelling. Essentially, the TGF activation theory stipulates that since SGLT2 inhibition also impedes sodium reabsorption at the PT, there should be increased distal sodium delivery to the macula densa and consequent attenuation of pathologic glomerular hyperfiltration. While these mechanisms may explain the nephroprotective effects of SGLT2is, the mechanism behind their beneficial role in heart failure is less clear.
A natural corollary of increased distal sodium delivery is natriuresis and therefore diuresis. This week’s NephJC article examines the diuretic properties of empagliflozin in patients with heart failure. Typically, volume status in patients with heart failure is managed with loop diuretics and adjuvant thiazide/thiazide-type diuretics (TZD). However, there are problems and limitations with these medications that SGLT2is may circumvent. Loop diuretics act directly on the macula densa to inhibit TGF, which exacerbates the maladaptive neurohormonal responses seen in heart failure (i.e., increased RAAS, adrenergic, and ADH system activation). Additionally, loop diuretics are less effective as extracellular fluid volume decreases (known as the “Braking Phenomenon”). This excellent Tweetorial by Aisha Shaikh provides further detail on these two problems with loop diuretics, which clinically manifest as diuretic resistance, a common challenge in heart failure treatment. The use of TZDs in heart failure, on the other hand, is limited by renal potassium and magnesium wasting, decreased uric acid excretion (increased risk of gout), and their propensity to cause a decline in renal function. The risks from thiazide induced hypokalemia were dramatically shown in this retrospective analysis by many of the same authors as our journal club article.
This week’s NephJC study looks at the effects of SGLT2is on natriuresis, volume status, and neurohormonal activation in patients with heart failure, in the acute and intermediate setting.
The Study
Methods
This is a randomized, double-blind, placebo-controlled, single center, cross over study. The study was investigator-initiated and registered on clinicaltrials.gov (NCT03027960).
Study Population
Inclusion criteria
Stable heart failure (HF) (diagnosed by an advanced HF cardiologist) defined by:
No hospitalizations during the preceding 60 days,
Stable HF medications for at least two weeks and stable diuretics for four weeks
Opinion of the HF cardiologist that the patient is at optimal volume status
Diagnosis of type 2 diabetes mellitus.
Regular home monitoring of blood glucose.
eGFR ≥ 45 mL/min/1.73m2.*
18 years of age or older.
*In an effort to improve enrollment rate, and given the cumulative safety experience gained in the ongoing large SGLT-2i trials, the eGFR inclusion criteria was modified to ≥ 20mL/min/1.73m2 in July 2018.
Exclusion criteria
The most important ones among the list are:
Active titration of chronic HF medications expected during the study period.
Use of a non-loop diuretic aside from an aldosterone antagonist (≤ 25 mg spironolactone or ≤ 50 mg eplerenone).
Critical stenotic valvular disease, complex congenital heart disease, or prior heart transplant.
History of diabetic ketoacidosis, brittle diabetes and/or frequent hypoglycemia, or severe hypoglycemic episodes requiring emergency intervention in the last 6 months
History of bladder dysfunction, incontinence, pyelonephritis, urosepsis, or frequent urinary tract infections
Anemia with hemoglobin < 8 g/dL
Intervention
Patients were randomized (permuted blocks randomization) to receive either 10 mg empagliflozin or matched placebo daily for 14 days followed by a two-week washout period and crossover to 14 days of treatment with the alternate therapy.

Here is the protocol used for body fluid space measurements and biospecimen collection on day 1 and 14:

Trial endpoints
Primary acute endpoint: natriuretic effect of empagliflozin both as a monotherapy and in combination with loop diuretics.
Primary 14-day endpoint: to understand if these acute natriuretic effects would translate into improved volume status after 14 days of therapy, as assessed by change in blood volume.
Secondary endpoints: change in neurohormones within 14 days of therapy.
A number of exploratory endpoints and biomarkers were also included to characterize the cardio-renal effects of empagliflozin in HF patients.
Other trial information
Fractional excretion of sodium (FENa) was the primary metric to describe sodium handling, chosen because it offers “the best instantaneous assessment of sodium excretion”.
eGFR calculated using the cystatin - and creatinine-based CKD-EPI equations.
Statistical analysis
To differentiate between two interventions over time: linear mixed model (LMM) with random intercepts, which incorporate correlated outcomes within-subject used, with 5% significance level cutoff.
To account for crossover design effect, the LMM was adjusted for the interaction between time and the order of the interventions.
Funding
The trial received both drug and financial support from Boehringer-Ingelheim Pharmaceuticals, Inc. Two of the authors have conflicts related to the company.
Results
A total of 21 patients were randomized in the study (11 receiving empagliflozin in Arm 1; 10 receiving empagliflozin in Arm 2, however one was excluded from final analysis due to medication noncompliance).

Of the 20 patients included in the final analysis:
75% were men with an average age of 60±12 years
BMI of 37±7 kg/m2.
median HbA1c:- 7.1%
8/20 (40%) were taking insulin at baseline
9/20 (45%) patients had HFrEF (EF <40%).
median daily home loop diuretic dose was 244 ± 306mg furosemide equivalents.
The peak FENa after receiving 1.9 ± 1.4 mg bumetanide during the placebo period was 3.9 ± 1.9% (normal response would be an increase in FENa of >20%).
The mean eGFR was 69.1±19mL/min/1.73m2, and 7/20 had an eGFR <60. See full table of baseline characteristics here.
Effect of empagliflozin on kidney glucose handling
As expected, there was a marked (27-fold) increase in urinary glucose excretion, which peaked 3 hours after initial administration of empagliflozin and was sustained after 14 days of treatment. Patients with a higher eGFR had much greater glucose excretion (p interaction=0.001).
Effect of empagliflozin on kidney sodium handling
A statistically significant natriuretic effect was observed with empagliflozin monotherapy (p<0.001) both during the Day 1 (p<0.001) and Day 14 (p=0.02) visits. The authors also report synergistic natriuresis following the administration of bumetanide.

Changes in volume status and red cell indices
Empagliflozin therapy resulted in a
greater reduction in total blood volume and plasma volume at Day 14.
Erythropoietin increased more in patients receiving empagliflozin at Day 14.
There was no significant change in the measured red cell volume and NT-proBNP between the empagliflozin and placebo group.
Effect of empagliflozin on potassium, magnesium, and uric acid handling
No significant difference was noted in the 6 hour potassium excretion and serum potassium level.
On day 1, there was a trend toward reduction in total urine magnesium excretion (3.8 ± 1.5 mmol vs. 4.6 ± 1.2 mmol, p=0.08) with empagliflozin, and the urine sodium to magnesium ratio substantially increased (95 ± 56 vs. 55 ± 23, p=0.002).
Empagliflozin therapy had a uricosuric effect which was surprisingly largest and significant when combined with loop diuretics (p<0.001).
There was no difference between urine urea concentration between empagliflozin and placebo.
Neurohormonal Activation and Inflammatory Biomarkers
Levels of plasma renin activity, total renin, and aldosterone were stable. The change in plasma norepinephrine levels was significantly less pronounced with the addition of empagliflozin compared to bumetanide alone (p=0.023). There were no differences in inflammatory biomarkers tested. Fasting ketone levels increased following 14 days of empagliflozin therapy vs. placebo (0.046 ± 0.131 mmol/L vs -0.012 ± 0.105 mmol/L; p=0.05). See the values for all biomarkers here.
Effects on glomerular filtration, tubular injury, and renal secretory capacity
There were no significant differences after 14 days of empagliflozin vs. placebo therapy for several measures of kidney function, including creatinine-based eGFR, cystatin C-based eGFR, β2-microglobulin concentration, six hour creatinine clearance, albuminuria and urine NGAL. The change in urine KIM-1 was significantly better during empagliflozin therapy [90 ng/mg of creatinine (IQR -514 to 1211)] compared to placebo [226 ng/mg of creatinine (IQR -132 to 894; p=0.023)].
Vital signs, electrolytes, and adverse events
Empagliflozin was well tolerated in this study. Specifically, there were no instances of genitourinary infections, symptomatic hypoglycemia, diabetic ketoacidosis. This was a short study with a small number of patients, so this is not unsurprising.
There was a significant change in patient weight and in calculated total body water after 14 days of empagliflozin treatment.

However, there were no significant differences in systolic blood pressure, diastolic blood pressure, mean arterial pressure or heart rate. There was no significant effect on serum sodium, bicarbonate, chloride, calcium and phosphorous levels.
Effect of empagliflozin on potassium, magnesium, and uric acid handling
No significant difference was noted in the 6 hour potassium excretion and serum potassium level.
On day 1, there was a trend toward reduction in total urine magnesium excretion (3.8 ± 1.5 mmol vs. 4.6 ± 1.2 mmol, p=0.08) with empagliflozin, and the urine sodium to magnesium ratio substantially increased (95 ± 56 vs. 55 ± 23, p=0.002).
Discussion
A natriuretic role for SGLT2i inhibitors has been postulated since at least 2016 (Rajasekeran et al., KI, 2016), given the observed benefits in HF and modest blood pressure improvement (SBP ↓4-6 mmHg per Perkins et al., AJKD, 2016) upon initiation of this class of drugs. Other possible mechanisms for SGLT2i-associated diuresis and BP lowering include passive glucose-induced osmotic diuresis and water diuresis via direct modulation of ADH system proteins.
Human data exploring these mechanisms are limited with mixed results. An early dapagliflozin randomized trial (n = 47 subjects) showed that it induced transient natriuresis, which had resolved by the 2 week time point (Komoroski et al., Clin Pharmacol Ther, 2009). This finding was recapitulated in a single-arm study of 13 patients receiving canagliflozin (Tanaka et al., Adv Ther, 2017). Significantly increased volume of urine output has been documented in patients with T1D and baseline kidney hyperfiltration (but not normofiltration); however there were no differences in urine sodium excretion over the 28-day study period (Cherney et al., Circulation, 2014). However, none of these studies were designed to quantify natriuresis or diuresis as the primary outcome, and uncontrolled factors (such as diet and fluid intake) might have biased these observations.
The authors of this small, mechanistic clinical trial examined the diuretic properties of empagliflozin in a controlled setting. They conclude that empagliflozin induces modest natriuresis in patients with type 2 diabetes and heart failure in its acute and intermediate phases of action. They describe this effect as synergistic with loop diuretic action (per Figure 3, empagliflozin increases FENa by a factor of 1.5 in each case). The observed decrease in blood and plasma volume was not accompanied by signs of RAAS or adrenergic system hyperactivation, nor by acute kidney injury. They conclude that “empagliflozin functions as a loop diuretic adjuvant with a clinically significant effect on natriuresis and what appears to be an excellent neurohormonal/renal/electrolyte safety profile”.
Strengths:
Addresses a timely question: What drives improved HF outcomes in patients taking SGLT2 inhibitors?
Thorough study examining several variables over many time points in a short period.
Limitations of the study listed by the authors:
Population studied: Small sample size, single centre, patients highly selected (stable, euvolemic HF patients only). Unclear if generalizable to non-diabetics.
Short study period: patients followed for 14 days so it is unlikely that sodium balance was re-established. Chronic natriuretic effect cannot be determined.
Fasting setting: Since patients were fasting pre-study, the effect of dietary sodium load on SGLT2i natriuresis efficacy is unknown.
Multiple other hypotheses proposed for SGLT2i benefit in HF – cannot be excluded and these other mechanisms remain in play.
Other limitations of the study:
Use of FENa: sodium excretion is exclusively reported as the FENa in this study, which normalizes sodium excretion based on creatinine excretion. SGLT2 inhibitors exert their renoprotective effect by decreasing glomerular filtration, and their initiation is often associated with a bump in serum creatinine. Since creatinine filtration is typically affected by SGLT2i initiation, FENa may not be a reliable measure of sodium excretion. Curiously, this 2-week study did not note a decrease in eGFR at SGLT2i onset.

Change in eGFR from baseline. Adapted Figure 3B from Perkovic et al., NEJM.
Incomplete reporting of intervention: The methods state that 12 patients consumed a sport drink (Gatorade) instead of receiving IV water with 5% dextrose (D5W). It is unclear which 12 patients received this and whether it was for one or both arms of the study. The 500 mL oral bolus of Gatorade contains ~230 mg of sodium and ~30 g of sugar, whereas the D5W IV bolus contains no sodium and 25 g of sugar. The different micronutrient content and modes of administration of these two fluids could significantly affect natriuresis and glucouresis. However, this is not accounted for in the study.
Conclusion
The benefits of SGLT2 inhibitors have been extended beyond their initial indication of glycemic control in diabetes. The mechanisms by which they improve outcomes in heart failure and kidney disease are being explored. The current study provides preliminary evidence for a natriuretic effect of SGLT2 inhibitors, observed at the onset of therapy in euvolemic patients already on loop diuretics.
SGLT2 inhibitors may be a safe adjuvant diuretic agent for volume control in HF patients. However, larger studies are needed to confirm this effect and examine how chronic SGLT2i use impacts salt and water homeostasis in this population.
Summary prepared by:
Caitlyn Vlasschaert
Department of Medicine, Queen’s University – Kingston, Ontario, Canada
Krishna K Agrawaal
Department of Nephrology, Universal College of Medical Sciences – Bhairahawa, Lumbini, Nepal