


Nephrology is plagued with a dearth of randomized controlled trials so when we get one randomized controlled trial (RCT) on a clinically relevant question we feast like kings, but when we get two RCTs on the same question in a week what do we do?
Actually, we have have no idea what we do. But this is where we find ourselves today with AKIKI and ELAIN both providing fresh RCT data on when to initiate dialysis in acute kidney injury (AKI).
Acute kidney injury has been a tough nut to crack. Despite decades of research and scores of studies mortlity in AKi has remained stubbornly elevated.

Am J Med 2005 118, 827-832
At the turn of the century, dose of dialysis was the target and higher dose was going to be the key to better outcomes with dialysis dependent AKI. This was definitively rejected by the ATN trial.

Now the question has moved from dose to timing, when should we use dialysis in AKI. Does starting dialysis early in AKI improve outcomes?
Dr. Faubel took up this question in her entirely hypothetical DreamRCT, NephroRULES. The first study to land was AKIKI. The issues were beautifully and succinctly summarized by the authors of the ELAIN study:
“Earlier initiation of RRT may produce benefits by avoiding hypervolemia, eliminating of toxins, establishing acid-base homeostasis, and preventing other complications attributable to AKI. However, early initiation of RRT may unnecessarily expose some patients to potential harm because some patients will spontaneously recover renal function.”
summarized
AKIKI
AKIKI is a French, multi-center, randomized, unblinded trial of early versus late dialysis. The basic structure of the study is patients were randomized to either early or late dialysis. The early patients were started on dialysis as soon after randomization as possible. The late dialysis cohort initiated dialysis when they crossed any one of a number of dialysis triggers.
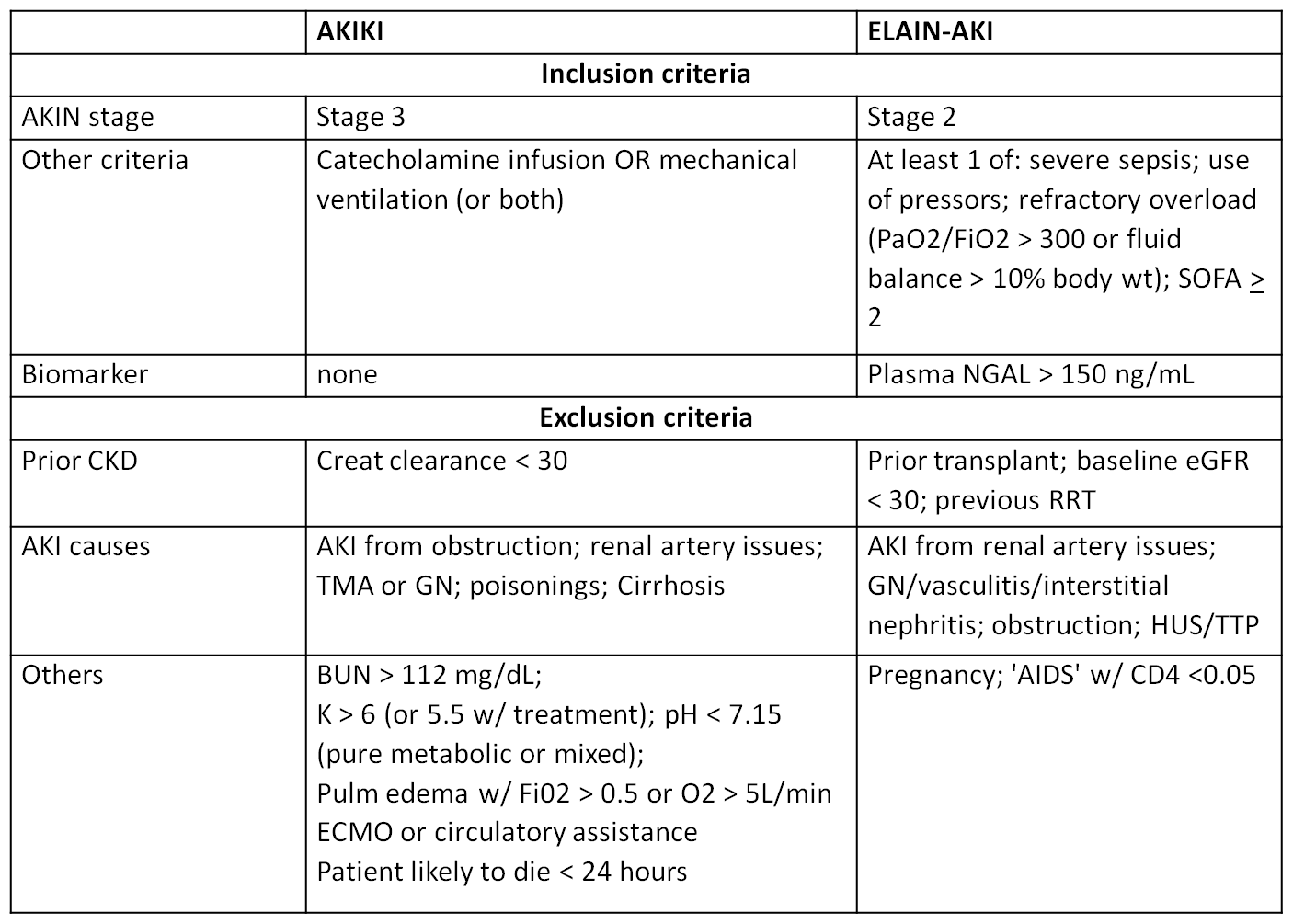
Inclusion criteria: patients were adults admitted to the ICU with AKI due to presumed acute tubular necrosis from either toxic or ischemic injury. All patients had KDIGO stage 3 acute kidney injury and were either intubated or on vasopressors.
The exclusion criteria are important because, in addition to being traditional exclusion criteria, they were later used as indications for initiating dialysis in the late start group.
Exclusion criteria:
BUN > 112 mg/dL
Potassium > 6 mmol/L (or > 5.5 despite medical treatment)
pH < 7.15 with either PaCO2 < 35 mm Hg or PaCO2 > 50 mm Hg without the possibility of increasing alveolar ventilation
Acute pulmonary edema due to fluid overload resulting in hypoxemia requiring an oxygen flow of 5 lpm to maintain sats ≥ 95% or FiO2 > 50% despite diuretic therapy
In addition to the above criteria the late group would also initiate dialysis if oliguria persisted longer than 72 hours.
“Would you dialyze a non-oliguric (35%) patient with a creatinine of 3.2, potassium of 4.4, BUN of 53, and bicarbonate of 18? You would if you enrolled them in AKIKI.”
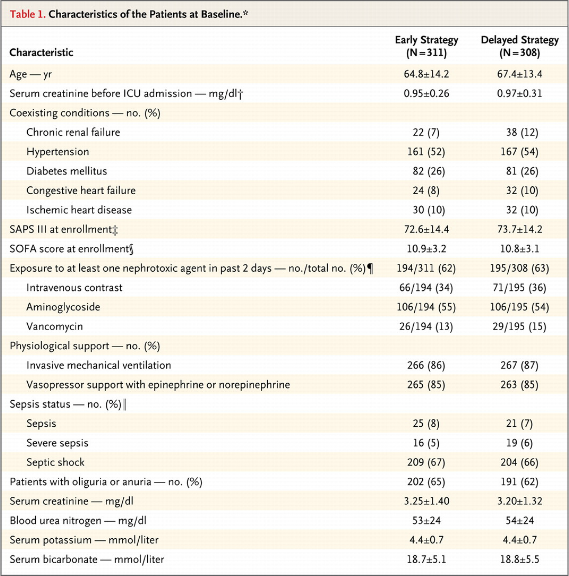
620 people were randomized, 312 in the early group and 308 in the delayed group. This was a sick cohort, 80% had sepsis. 85% were on vasopressin and a similar fraction was intubated.
In the early group the first dialysis was started at a mean of 4.3 hours after documentation of AKI stage 3. In the late group, of the 308 patients, only 157 ever received dialysis and they initiated at a mean of 57 hours. The most common indications for dialysis was a BUN of 112 and oliguria for 72 hours.
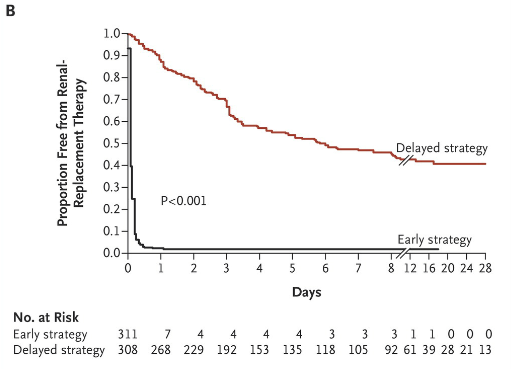
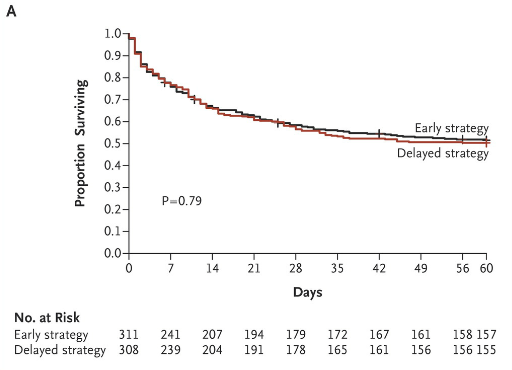
Bottom line: Mortality was the same between the two groups. There were 303 deaths by 60 days after randomization, 150 in the early initiation cohort, 153 in the late initiation cohort. Late dialysis had the same mortality with half as much dialysis as the early start cohort.
ELAIN Trial
The second half of this bounty of RCTs is ELAIN. This was a single-center, pilot study.
The inclusion criteria here was KDIGO Stage 2 AKI.
Patients also needed:
plasma neutrophil gelatinase–associated lipocalin (NGAL) >150 ng/mL
At least 1 of the following conditions: severe sepsis, use of vasopressors or catecholamines (norepinephrine or epinephrine >0.1 μg/kg/min), refractory fluid overload (worsening pulmonary edema, PaO2/FiO2 <300 mm Hg or fluid balance >10% of body weight), development or progression of nonrenal organ dysfunction (Sequential Organ Failure Assessment [SOFA] score ≥2)
Age between 18 and 90 years
Intention to provide full intensive care treatment for at least 3 days.
The exclusion criteria:
Preexisting chronic kidney disease stage 4 or 5, previous renal replacement therapy, AKI caused by permanent occlusion or surgical lesion of the renal artery, glomerulonephritis, interstitial nephritis, vasculitis, post-renal obstruction, or hemolytic uremic syndrome or thrombotic thrombocytopenic purpura were excluded. We also excluded patients for pregnancy, prior kidney transplantation, hepatorenal syndrome, AIDS, hematologic malignancy with neutropenia.
The intervention:
Patients randomized to the early group started dialysis within 8 hours of enrollment in the study. Patients in the late group initiated dialysis within 12 hours of progressing to KDIGO Stage 3 AKI or develop an absolute indication for dialysis which they listed as:
- serum urea level higher than 100 mg/dL
- serum potassium higher than 6 mEq/L and/or with electrocardiography abnormalities
- serum magnesium level higher than 8 mEq/L (to convert to mmol/L, multiply by 0.5)
- urine production lower than 200 mL per 12 hours or anuria
- organ edema in the presence of AKI resistant to diuretic treatment
All patients received CRT.
Results:
They randomized 231. The early group had 112 and the late group 119. Everyone on the early group was dialyzed, however only 89% of those in the late group ultimately received dialysis due to various reasons including recovery of renal failure.

The median time from meeting full eligibility criteria for RRT initiation in the early group was 6.0 hours compared to 25.5 hours for the late group.
The survival was significantly better with early initiation of dialysis, HR 0.66 (CI 0.045 to 0.97).

early dialysis also resulted in more renal recovery at day 90, reduced duration of mechanical ventilation, and decreased length of hospital stay.

So obviously the ELAIN study had dramatically different results from the AKIKI trial. Two things immediately come to mind, one the ELAIN trial initiated dialysis earlier that in AKIKI and then the patients received CRT. The ELAIN trial was a pilot study and given the discrepancy between the two studies I think it is safe to say that we will be waiting for the larger study before closing the book on the timing of dialysis initiation.