

#NephJC chat
Tuesday April 12th 2016, 9 pm Eastern
Wednesday April 13th 8 pm BST, 12 noon Pacific
N Engl J Med. 2016 Mar 10;374(10):940-50. doi: 10.1056/NEJMoa1508380.
Survival Benefit with Kidney Transplants from HLA-Incompatible Live Donors.
Orandi BJ, Luo X, Massie AB, Garonzik-Wang JM, Lonze BE, Ahmed R, Van Arendonk KJ, Stegall MD, Jordan SC, Oberholzer J, Dunn TB, Ratner LE, Kapur S, Pelletier RP, Roberts JP, Melcher ML, Singh P, Sudan DL, Posner MP, El-Amm JM, Shapiro R, Cooper M, Lipkowitz GS, Rees MA, Marsh CL, Sankari BR, Gerber DA, Nelson PW, Wellen J, Bozorgzadeh A, Gaber AO, Montgomery RA, Segev DL.
PMID: 26962729 Link to free full text, courtesy of NEJM.
Also see: Editorial in NEJM
Summary
Introduction and a bit of background
The survival benefit of receiving a renal transplant over remaining on the transplant waiting list is not in question. Wolfe et al (NEJM 1999) performed an excellent longitudinal study of 228,552 patients with end-stage kidney disease receiving hemodialysis and compared the survival of three patient groups; patients receiving a transplant (23,275), patients remaining on the waiting list (46,164) and patients deemed not fit for transplantation who continued on dialysis. They found (not unexpectedly) that mortality was 68% lower for patients receiving a renal transplant than for those remaining on the transplant waiting list. This represented a projected increase in mean survival of 10 years. This increased survival benefit was seen in both sexes, all age groups, and in patients with diabetes. The largest survival benefit accrued to dialysis patients who were younger, white and had diabetes.
A limited number of organs is the primary limiting factor preventing most people from being transplanted, however patient factors such as presence of anti-HLA antibodies play a significant role in lengthening transplant wait-list time. HLA molecules are the primary mechanism by which the immune system identifies self from non-self. They are essential to responding to commonly encountered viruses and bacteria, but are the prime mover in the allograft rejection response.
‘Sensitization’ is the process by which exposure to non-self HLA antigens leads to the formation of anti-HLA antibodies, which commonly occurs following:
blood transfusion
solid organ transplant
pregnancy
It is estimated that around 15% of wait-listed candidates have some degree of sensitization, with high levels of sensitization associated with longer wait times and increased likelihood of dying while on the waiting list. Sensitized patients have fewer options, but could potentially elect to participate in paired kidney donation or undergo desensitization therapy (of which there are several regimens) with incompatible transplantation. Outcomes from live-donor incompatible transplants are inferior to live-donor compatible transplants, but because HLA incompatibility is not accounted for in the case-mix reported from transplant centers, there is concern that centers may be discouraged from undertaking HLA incompatible transplants for fear of adversely affecting overall individual center outcomes.
This trial aimed to determine whether there was a survival benefit to undergoing desensitization and live-donor incompatible transplantation, compared to matched controls who remained on the waiting list, or who underwent deceased donor transplantation.
Methods
Adult patients who underwent kidney transplantation from HLA-incompatible live donors (defined as subjects undergoing perioperative desensitization therapy for donor-specific antibodies detected before transplant) were recruited from 22 centers in the United States between 1997 and 2011. Importantly, the centers involved were not just those who do large numbers of incompatible transplants. Indeed one of the points of this trial was to see if the results of a single center study (at Johns Hopkins University) were generalizable to centers that perform smaller numbers of incompatible transplants. Each center classified donor-specific antibody (DSA) level as low (positive Luminex assay with negative flow-cytometry), moderate (positive flow-cytometry with negative cytotoxic cross-match), or high (positive cytotoxic cross-match) (table 1).
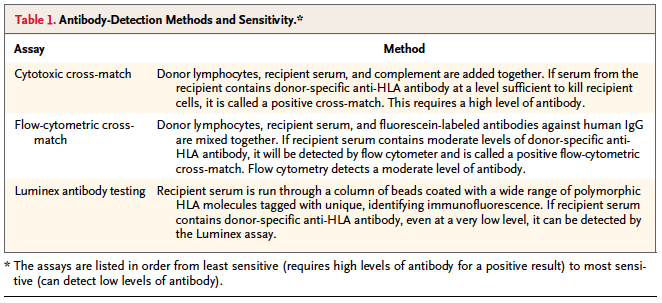
Table 1 from Orandi et al, NEJM 2016
Two sets of matched controls were drawn from the Scientific Registry of Transplant Recipients (SRTR): The first control group consisted of wait-listed patients, some of whom received a deceased donor transplant; the second group included wait-listed patients who remained on the waiting list and who never received a transplant. Five control patients for each control group were drawn from the SRTR registry for each incompatible transplant recruited.
The study went to great lengths to ensure controls were well matched, using ‘an iterative expanding-radius matching algorithm’ (a method that the authors had used before). Patients were matched for:
age
sex
race
previous renal transplant
donor age
duration of renal replacement therapy
diabetes mellitus
panel reactive antibodies.
The survival for all groups were compared using Kaplan-Meier analyses.
Results
1,025 patients who received a kidney transplant from an incompatible live donor were recruited: 185 with ‘low’ antibody levels, 536 with ‘moderate’ antibody levels and 304 with ‘high’ antibody levels (details in table 2). There were more female patients in each group (67% female overall), and the control groups were well matched (table 3). Whilst there were some differences between the groups that reached statistical significance, they seem clinically negligible:
The mean age of the incompatible transplant group was 45.0 years compared to 46.6 years in the control group who remained on the waiting list and never underwent transplantation (P=0.001)
the antibody incompatible group were more likely to have had a previous transplant than both the wait-list/transplant group (P=0.004) and the wait-list-only group (P=0.02). \
Patient follow-up data up extended out to to 8 years.

Table 3 from Orandi et al, NEJM 2016
There was a significant survival advantage for recipients of kidney transplants from incompatible live donors compared to both patients in the wait-list only and the wait-list/transplant group (figure 1).

Figure 1 from Orandi et al, NEJM 2016
The survival advantage existed at 1, 3, 5 and 8 years (table 4, also see below). Overall, receiving an incompatible kidney transplant conferred an absolute increase in survival rate at 8 years of 13.6%, compared to remaining on waiting list or receiving a deceased donor transplant (Risk of death reduced by a factor of 1.83; 95% CI 1.58 – 2.12, P<0.001), and an absolute increase in survival rate of a whopping 32.6% compared to remaining on the waiting list ( risk of death reduced by a factor of 3.37; 95% CI 2.92 – 3.9, P<0.001) – Yes, those are some impressive figures!

This survival advantage was seen in patients with low, moderate and high donor specific antibody levels (figure 2)

Figure 2 from Orandi et al, NEJM 2016
Discussion
There have been several press-release commentaries accompanying this article, including from the New York Times, Richard Lehman (whose quote we use in the title), Johns Hopkins, NEJM Journal Watch and Renal and Urology News (@RenalandUrology) and most recently, Drs Berns and Sawinski on Medscape.
This was an excellent study that sought to answer the question ‘Is there a survival benefit to receiving a live related incompatible transplant compared to staying on the waiting-list and/or receiving a deceased donor kidney’ and the answer seems to be a resounding yes! The trial not only supports previous work, but because of it’s multicenter design, suggests the results are generalizable to most transplant centers – not only those who do a large number of antibody incompatible transplants. Although not in the main article it was also encouraging to note that survival rates were similar across all participating centers, regardless of the volume of transplants done. The study design is to be commended for selecting a wait-list/transplant group as a control group, (rather than just a waiting-list control group, or even a matched control group who may or may not remain on the waiting-list), as this is the next best real-world alternative.
The desensitization regimens, induction and maintenance immunosuppressive regimens and treatment strategies for rejection varied between centers. While some may see this as a weakness, I believe this to be a strength that enhances the generalizability of the survival benefit seen from receiving an incompatible transplant. No doubt the most appropriate desensitization regimens for the varying degrees and types of DSA will be argued about following future trials designed to assess these specifically, but that is for another day.
Managing these patients is still tricky and there are a number of serious side effects of desensitization therapy and increased risk of organ failure (compared to compatible live donor transplants) that mean incompatible transplants should not be undertaken lightly. That said, this study suggests that for those facing a long (and possibly interminable) wait for deceased donor match due to DSA, there is now strong evidence that for many patients these risks are worth taking for a considerable survival benefit.
Summary prepared by Matt Graham-Brown, @drmattgb
#NephJC chat
Tuesday April 12th 2016, 9 pm Eastern
Wednesday April 13th 8 pm BST, 12 noon Pacific