
Finerenone in Type 1 Diabetes and Chronic Kidney Disease
N Engl J Med, March 4, 2026. DOI: 10.1056/NEJMoa2512854
PMID: 41780000
WHY WAS THE STUDY DONE?
Type 2 diabetes accounts for >85% of patients diagnosed with diabetes.The management of diabetic kidney disease has been built on a narrow foundation comprising glycemic control, blood pressure optimization, and renin–angiotensin system blockade, yet residual CKD risk has been stubbornly high. While patients with type 2 diabetes have enjoyed a renaissance of therapies to address these residual risk, with SGLT2Is, GLP-1 RAs, and nsMRAs (finerenone), patients with type 1 diabetes have largely been left behind and excluded from these groundbreaking studies of newer therapeutics. Flozins of course have been tried and sotagliflozin caused ketoacidosis (Garg et al NEJM 2017).
Figure 1. Mechanism of renal-cardio damage by Mineralocorticoid Receptor activation from Ruolin et al, Front Endocrinol 2023
Activation of the mineralocorticoid receptor drives sodium retention and promotes renal inflammation, oxidative stress, and fibrosis, accelerating injury in diabetic kidney disease (DKD). Nonsteroidal MRAs (nsMRA) supposedly selectively block this pathway, suppressing pro-inflammatory and pro-fibrotic signaling and slow structural kidney damage beyond their modest hemodynamic effects.
Figure 3: Inhibition of MR overactivation by finerenone from Arici et al, Front Med 2024
Several large studies have shown the worth of nsMRAs in patients with Type 2 diabetes. FIDELIO-DKD demonstrated a significant reduction in kidney failure and CV outcomes (HR 0.82 for the primary kidney composite), complemented by FIGARO-DKD and consolidated in the FIDELITY pooled analysis, which showed a 23% reduction in major kidney outcomes and a consistent effect across CKD stages. Mechanistically, these benefits appear tightly linked to albuminuria reduction (Agarwal et al, Annals of IM 2023). Early declines in UACR accounted for up to 84% of kidney protection with finerenone. This reinforced albuminuria as both a therapeutic target and a surrogate endpoint. This is the rationale for FINE-ONE attempting to translate a well-established T2D paradigm into the long-neglected space of DKD in patients with type 1 diabetes.
HOW WAS THE STUDY DONE?
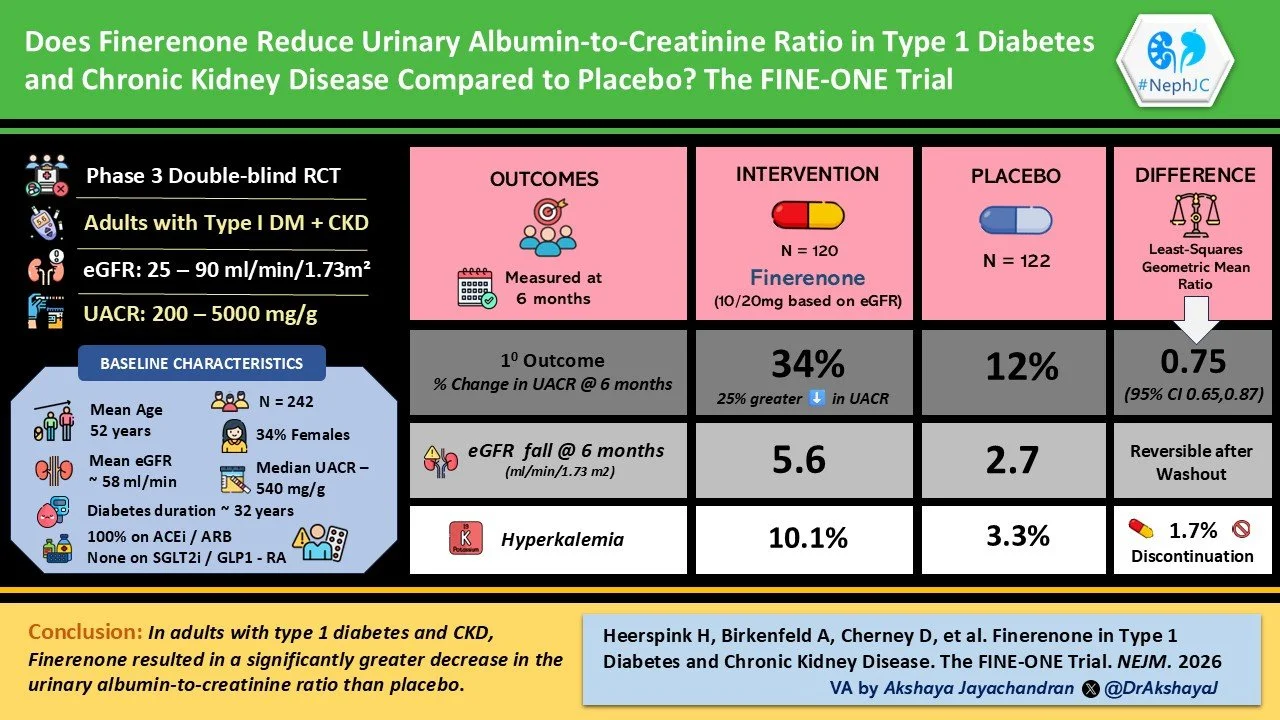
FINE-ONE included adults (≥18 years) with type 1 diabetes and chronic kidney disease. The eGFR cut-off for inclusion was between 25 to <90 ml/min/1.73 m² along with albuminuria (UACR 200 to <5000 mg/g). The proteinuria had to be documented for at least 3 months prior to screening. All participants were required to be on a stable dose of an ACE inhibitor or ARB for at least 4 weeks before enrollment. Additional inclusion criteria included HbA1c <10% and serum potassium ≤4.8 mmol/L at screening. Key exclusions included CKD due to causes other than type 1 diabetes, prior kidney transplantation, symptomatic heart failure with reduced ejection fraction, and recent use of flozins or GLP-1 RAs.
Participants were randomized 1:1 to receive finerenone or placebo. If eGFR was ≥60 ml/min/1.73 m², the starting dose was 20 mg once daily, and it was 10 mg daily in those with eGFR 25 to <60 ml/min/1.73 m². Dose reduction or temporary discontinuation was allowed for safety, particularly in the setting of hyperkalemia. The trial was double-blind, and all participants continued RAS blockade.
The primary outcome was the relative change in UACR from baseline over 6 months. Secondary outcomes were: Changes in eGFR, serum potassium, Blood pressure and adverse events, including hyperkalemia. Exploratory outcomes included categorical reductions in UACR (≥30% and ≥50%).
WHAT DID THE STUDY FIND?
A total of 573 participants were screened, and 242 were randomized: 120 to finerenone and 122 to placebo. Treatment discontinuation during the 6-month period occurred in 6.7% of the finerenone group and 8.2% of the placebo group. As expected, UACR fell by 34% in the finerenone group vs 12% in the placebo group, translating to a 25% greater fall with nsMRA treatment. More than half of patients on finerenone achieved at least a 30% (with ⅓ achieving a 50% decline in UACR) reduction in albuminuria vs only 29% in the placebo arm.
Figure 2. Change in the Urinary Albumin-to Creatinine Ratio According to Subgroup from Heerspink et al, NEJM 2026
There was a greater decline in eGFR in the finerenone group of about −5.6 ml/min/1.73 m² at 6 months compared with −2.7 in the placebo group, giving a between-group difference of −2.9. This separation appeared early and then stabilized, and during the washout period eGFR in the finerenone arm moved back toward baseline. A decline of 30% or more in eGFR was seen in 9.2% of patients on finerenone and 7.4% on placebo.
Blood pressure changes were minimal, and there was no meaningful change in glycemic control or body weight over the course of the study.
Figure 3. Changes in Potassium, eGFR and Systolic and Diastolic Blood Pressure from Heerspink et al, NEJM 2026
Adverse events were broadly similar between the two groups, both in overall frequency and in serious events. What stood out, as expected, was hyperkalemia. It occurred in about 10% of patients receiving finerenone compared with just over 3% in the placebo group, and around 2% had to stop the drug because of it. There were no deaths in the finerenone group during the trial. Hypoglycemia was actually less frequent with finerenone than with placebo, though the numbers were small.
ARE WE IMPRESSED ?
So, FINE-ONE answers a question we have been circling for years. If MR activation matters in type 1 DKD, will blocking it actually do anything? The trial shows that it does. Albuminuria comes down. It comes down clearly and consistently over 6 months. That part is straightforward.
But once you move beyond that, things get a bit less clear. This is a trial built around albuminuria, and not kidney failure, long term eGFR decline, or dialysis. Just albuminuria. It is considered a useful marker, no doubt, but it is still far from outcomes that these fairly young and long-standing diabetic patients actually feel. The expectation is that lowering this number will translate into something bigger later on.
The eGFR story adds to that uncertainty. There is a drop early on with finerenone, larger than placebo, and then some recovery after stopping the drug. It looks like a hemodynamic effect. We have seen this pattern before with other kidney drugs. It is not alarming, but doesn’t show what happens over long follow-ups. The trial is also short. Six months is enough to show that a drug changes a number. It is not enough to show that it changes the course of a disease. The authors do mention that the curves look stable and suggest longer follow up may not change things much. However, kidney outcomes take time, sometimes a lot of time. Given the smaller number of patients, an outcome based trial may not be feasible, leaving us with this as the best available data.
Then there is the population itself. Out of 573 screened patients, more than half did not make it into the trial. That is a large number. The paper does not really break down why in detail. We know the criteria were strict. Potassium had to be low. Glycemic control had to be reasonable. Blood pressure couldn’t be too high or too low. No recent cardiovascular issues. No newer drugs (i.e., SGLT2i, GLP-1RA which are being used in selective patients with type 1 diabetes). This limits generalizability and does not mirror most of the type 1 diabetes patients seen in nephrology practice. One thing they did do well is handle missing data. The appendix goes into detail about how they imputed values and tested different assumptions. The results stayed consistent, which is reassuring. Safety looks like what we expect. More hyperkalemia with finerenone, not dramatic, but there. Otherwise, things are fairly similar between groups.
So what do we take away from all this?
Right now, this feels like an early step. A good one, but still an early one. All patients with diabetes differ, and diabetic DKD is not a monolith. Ongoing testing of newer DKD agents in patients with type 1 diabetes is essential to evidence based care (e.g., SUGARNSALT trial)
CONCLUSION:
Finerenone significantly reduces albuminuria over 6 months in patients with type 1 diabetes and CKD compared to placebo, with a modest and reversible decline in eGFR and a higher incidence of hyperkalemia. FINE ONE provides reassuring data when considering nsMRAs in patients with type 1 diabetes. Is this enough to start using finerenone in DKD due to type 1 diabetes - taken together with the T2D data from FIDELITY? Given the lack of other options in this patient population, that is a very sweet suggestion.