

#NephJC Chat
Tuesday October, 8th, 2024 at 9 pm Eastern (AEST = October 8th,11 am)
Wednesday October, 9th, 2024, at 9 pm by Indian Standard Time and 3:30 pm GMT (AEST = October 9th, 2 am)
Nature Med, 2024 Sep 1. doi: 10.1038/s41591-024-03264-4. Online ahead of print
Finerenone in heart failure and chronic kidney disease with type 2 diabetes: FINE-HEART pooled analysis of cardiovascular, kidney and mortality outcomes
PMID: 39218030





Introduction
For many patients, the classic risk factors for chronic kidney disease (CKD) are the exact same as cardiovascular disease (CVD). As your risk for CKD increases so does your risk for cardiovascular events and mortality. Thus, many of the goal-directed medical therapies (GDMT) for CKD overlap with heart failure and CVD treatments. The cardiovascular-kidney-metabolic (CKM) syndrome which includes diabetes, hyperlipidemia, hypertension, CKD, and CVD, has been garnering much attention in GDMT as of late (Ndmule et al, Circ 2023). The co-existence of these conditions puts patients at considerable risk of high medical expenditure as well as increased morbidity and mortality. It is postulated that CVD, CKD, and metabolic conditions share a common pathophysiological pathway (involving a hyperaldosterone state and end-organ fibrosis), and thus certain therapies may be beneficial across the spectrum of CKM.
Sebastian et al. Curr Probl Cardiol, 2024.
In this regard, the non-steroidal mineralocorticoid antagonist (ns-MRA), finerenone, has been under the spotlight for its favorable effects on cardiovascular health. The following picture illustrates the effect of mineralocorticoids on fluid and electrolytes, cardiovascular health, renal tissue, and tissue repair.
Mechanisms of cardiac and kidney damage induced by aldosterone excess, Chung EYM et al. Cochrane Library, 2024
In the RALES (Pitt et al, NEJM 1999), EPHESUS (Pitt et al NEJM 2001) , and EMPHASIS (Zannad et al, NEJM 2011) trials, in patients with heart failure with reduced ejection fraction (HFrEF), mineralocorticoid antagonists (MRAs) were associated with reductions in all-cause mortality and hospitalizations. Unfortunately, spironolactone and eplerenone were only noted to have a variable beneficial effect in heart failure with preserved ejection fraction (HFpEF). In fact, the TOPCAT trial (Pitt et al NEJM 2014) only showed benefits in the North American cohort, but was plagued by a significant failure to adhere to the study protocol in Russia and Georgia (see Pfeffer and Pitt, NEJM Evidence 2022). The use of MRAs is not without risk, and prescribing MRAs in CKD has always been precluded by the expectant risk of hyperkalemia and potentially worsening of eGFR. In addition, MRAs have anti-androgenic effects including gynecomastia, dysmenorrhea, and erectile dysfunction. In this context, ns-MRAs might have a more favorable risk to benefit profile. More recent data from FIGARO, FIDELIO (NephJC summary| Podcast), grouped together as FIDELITY have suggested additional benefits of ns-MRAs in slowing CKD and decreasing CV events in patients with advanced CKD and proteinuria specifically in the setting of diabetes. Do the benefits of finerenone extend beyond proteinuric diabetic kidney disease? The HFpEF nut in particular has been hard to crack (see TOPCAT discussion above) and only recently have PARAGON-HF (Solomon et al, NEJM 2019), and the flozin trials (EMPEROR PRESERVED; Anker et al NEJM 2021 and DELIVER; Solomon et al NEJM 2022) recently reported benefit, mostly driven by HF hospitalization, Into this area, finerenone recently walked in with the FINEARTS-HF trial (Solomon et al NEJM 2024), reporting a benefit, to no one’s surprise. However, how should one think of the renal benefits while adding this piece of information to the FIDELITY (aka FIDELIO + FIGARO) data? That is the aim of the FINEHEARTS analysis - a prespecified pooled analysis of the FIDELIO, FIGARO and FINEARTS HF trials.
The Study
Methods
The FINEHEART pooled analysis was a pre-specified, participant-level analysis of three phase 3 global, multi-center, double-blind, placebo-controlled randomized clinical trials of finerenone: FIDELIO, FIGARO, and FINEARTS-HF.
Search strategy for trial selection
Besides the above-mentioned practice-changing trials, a literature search of PubMed and MEDLINE was conducted to ensure no relevant trials of finerenone were missed. The strategy was as follows:
Extended Data Fig 1. Systematic Literature search. Vaduganathan et al. Nat Med, 2024.
Pooling Strategy and Sample size
Data was accessed at the individual participant level and pooled with harmonized data elements for baseline characteristics and clinical outcomes. Due to critical violations of “Good Clinical Practice,” 196 participants were excluded from all safety and efficacy analyses, resulting in a final sample size of 18,991 participants.
Pooled analysis outcomes definition
Efficacy outcomes were determined under intention-to-treat principles..
Safety outcomes were determined on the basis of patients having taken at least one dose of finerenone..
Treatment-emergent adverse events collected included hyperkalemia, acute kidney injury, hypotension, and gynecomastia in any patient who has received at least one dose of the study drug and within 3 days of permanent discontinuation, including during periods of temporary drug interruption.
The primary outcome of the study was time to cardiovascular death, with secondary outcomes including a kidney composite outcome, hospitalizations, and major adverse cardiovascular events (MACE).
Statistical Analysis
Primary and secondary outcomes were analyzed using stratified Cox proportional hazards and considering the study intervention group as a fixed effect; stratified by geographic region and individual trial. Kaplan-Meier curves were used for selected outcomes presented as Kaplan-Meier curves. Secondary outcomes were tested regardless of primary outcomes results, with no multiple testing strategy.
Pre-specified sensitivity analysis was performed for the primary outcome, considering deaths of undetermined causes in all 3 trials as cardiovascular deaths.
The pre-specified statistical plan was registered on PROSPERO before unblinding FINEARTS-HF. All trials were assessed as high quality with a low risk of bias prior to pooling.
Funding
All trials included in the pooled analysis were funded by Bayer AG. Trial steering committees, along with the sponsor, designed and oversaw trial conduct, however, had no role in analysis, interpretation of data, and manuscript drafting. Five of the authors are Bayer employees and most of the other authors have ties to Bayer.
Results
The study analyzed 18,991 participants to evaluate the safety and efficacy of finerenone versus placebo. Baseline characteristics of patients from individual trials is as follows.
Table 1. Baseline Characteristics FINE-HEART. Vaduganathan et al. Nat Med, 2024.
Mean age of participants was 67 (± 10) years and 35.1% were females. Participants represented all major geographical regions. A significant proportion of the participants were considered high-risk for CKD progression; up to 30% of participants had an eGFR less than 45 ml/min/1.73m2 (driven by FIDELIO-DKD) and 49.2% had urinary albumin creatinine ratio (UACR) >/= 300mg/g (A3). While over 90% of the patients were on ACEi, ARBs or ARNI, less than 10% were on SGLT2i or GLP-1RA. The use of flozins went up with time, but notably, the use of GLP-1RA was lowest in FINEARTS, reflecting the lower proportion of patients with diabetes. The use of potassium-lowering therapies was higher in FIDELIO-DKD than in the other two trials.

Adapted from Extended Data Table 4. Baseline characteristics by trial. Vaduganathan et al. Nat Med, 2024.
Finally, 12% participants had all three CKM conditions (HF, CKD, and DM), and 90% with at least 2 conditions, FINEARTS-HF included patients with a LVEF >40%, but this was not specifically measured in the other pooled studies (FIGARO and FIDELIO). The median follow-up of the pooled population was 2.9 years.
Extended Data Fig 3. CKM Overlap in FINE-HEART. Vaduganathan et al. Nat Med, 2024.
Primary outcome: cardiovascular deaths
The primary endpoint of cardiovascular death occurred in 421 (4.4%) of participants in the finerenone arm and in 471 (5%) of participants in the placebo arm Hazard Ratio (HR) 0.89; (95%CI: 0.78–1.01).
Figure 2a. Cumulative incidence of death. Vaduganathan et al. Nat Med, 2024.
Effects on cardiovascular death were also consistent across individual trials. (Pinteraction = 0.68)
Extended Data Fig 4. Key Efficacy Outcomes in Each trial. Vaduganathan et al. Nat Med, 2024.
Renal outcomes
Finerenone reduced the risk of a sustained decrease in eGFR to ≥50% from baseline (HR: 0.80; 95% CI: 0.72–0.90) or to ≥57% from baseline (HR: 0.79; 95% CI: 0.70–0.91) - see extended data figure 4.

Figure 2c. Composite kidney outcomes. Vaduganathan et al. Nat Med, 2024
Risk of hospitalizations
The risk of hospitalization due to HF was lower with finerenone. (HR: 0.83; 95% CI: 0.75–0.92).
All-cause hospitalizations were also lower with finerenone compared to placebo. (HR: 0.95; 95% CI: 0.91–0.99).

Figure 2b. Cumulative incidence of HF Hospitalization. Vaduganathan et al. Nat Med, 2024.
Treatment effect on CV health across HF/CKD/DM conditions
Treatment effects were consistently non-significant across the range of CKM disease burden:
One condition (HR: 0.93; 95% CI:0.65–0.1.33)
Two conditions (HR: 0.87; 95% CI: 0.74–1.03)
Three conditions (HR: 0.91; 95% CI: 0.71–1.18)
P interaction = 0.94
Figure 2d. Cumulative incidence of All-cause Death. Vaduganathan et al. Nat Med, 2024.
Specific causes of death including CV and non-CV can be seen in Table 2. CV causes of death are lower (p is NS given low numbers) but it is useful to see that non-CV causes of death (mostly infections and trauma) are similar between arms.
Table 2. Cause of death. Vaduganathan et al. Nat Med, 2024.
The incidence of any serious adverse event was lower with finerenone than with placebo (34.6% versus 36.6%), although there was a higher incidence of hyperkalemia (1.3% vs 0.5%) and hyperkalemia-related hospitalizations (0.8% vs 0.2%), without any deaths related to hyperkalemia. The incidence of serious adverse events leading to drug discontinuation was slightly higher with finerenone (5.4% versus 4.6%). There were no significant differences in the incidence of acute kidney injury between groups.

Table 3. Adverse events. Vaduganathan et al. Nat Med, 2024.
Discussion
In this prespecified pooled analysis, FINEHEART reported consistent beneficial effects of finerenone across a wider range of population for most cardiorenal outcomes of interest.
Key Strengths
FINE-HEART is the largest participant-level pooled analysis examining an ns-MRA, pulling together the data from three trials that FIGAROously expanded the participant pool, capturing a broad spectrum of patients across CKM conditions. While FIGARO and FIDELIO focused on patients with CKD and diabetes, FINEARTS-HF was more inclusive, with around 60% of participants not having diabetes or CKD, though ~ 60% did not have significant albuminuria. All the trials had excluded patients with reduced ejection fraction.
Key Limitations
Strict inclusion and exclusion criteria across the trials mean the results might not generalize to all patient populations. Black participants, for example, were underrepresented, which limits the applicability to this demographic. Also, not every data element was collected uniformly across the trials. For instance, urgent HF hospital visits were only recorded in FINEARTS-HF, but not in the diabetic CKD trials. The low proportion of patients with SGLT2i and GLP-1RA (less than 10%) further complicate the ability to make concrete claims about finerenone’s additive effects with newer therapies.
So what, if anything, does FINEHEART add to our knowledge and comfort with using ns-MRAs in patients with CKM? The study population of FINEHEART included nearly 20% of patients without CKD or diabetes, and approximately 60% without heart failure or proteinuria in both the treatment and placebo arms. There was an attempt to harmonize data elements for baseline characteristics and clinical outcomes between the three pooled studies, leading to a heterogeneity not seen in any individual study. For example, FIDELIO specifically excluded patients with symptomatic HF or reduced EF, while FINEART-HF exclusively enrolled symptomatic HF patients. It is these widely varied participants that give us a much broader view of where ns-MRAs could potentially be of benefit.
FINEHEART once again showed the kidney benefits of ns-MRA in slowing eGFR decline, showing a reduction in the kidney composite outcome by 20%, driven primarily by benefits previously observed in FIDELIO-DKD and FIGARO-DKD. Indeed, FINEARTS HF did not report a renal benefit on its own (75 renal composite events with finererone versus 55 in placebo). Thus the cynical take would be that FINEHEARTS is attempting to soften this blow from FINEARTS HF.
No new or unexpected safety signals were uncovered in this pooled analysis with a well-characterized modestly higher (expected) risk of hyperkalemia with finerenone. The diverse spectrum of benefits underscores the systemic actions of finerenone in attenuating adverse multi-organ effects of mineralocorticoid receptor overactivation and moderating inflammation and fibrosis across multiple organs. The wealth of data on the usefulness of ns-MRAs continues to grow, yet many of us are still left wondering if older, cheaper MRAs are just as beneficial. Does anyone want to fund a ns-MRA versus MRA study? (I’ll check my couch cushions).
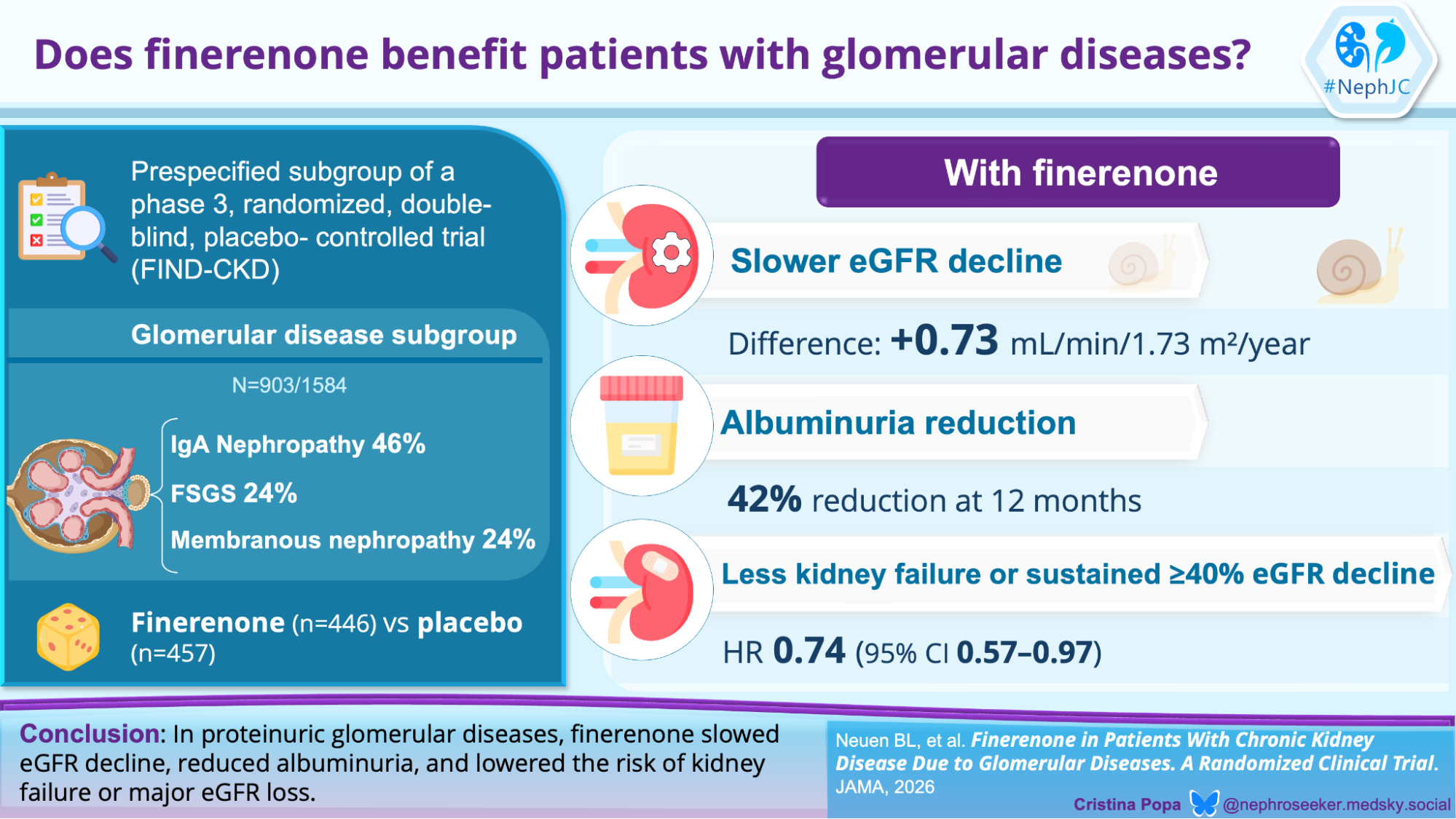
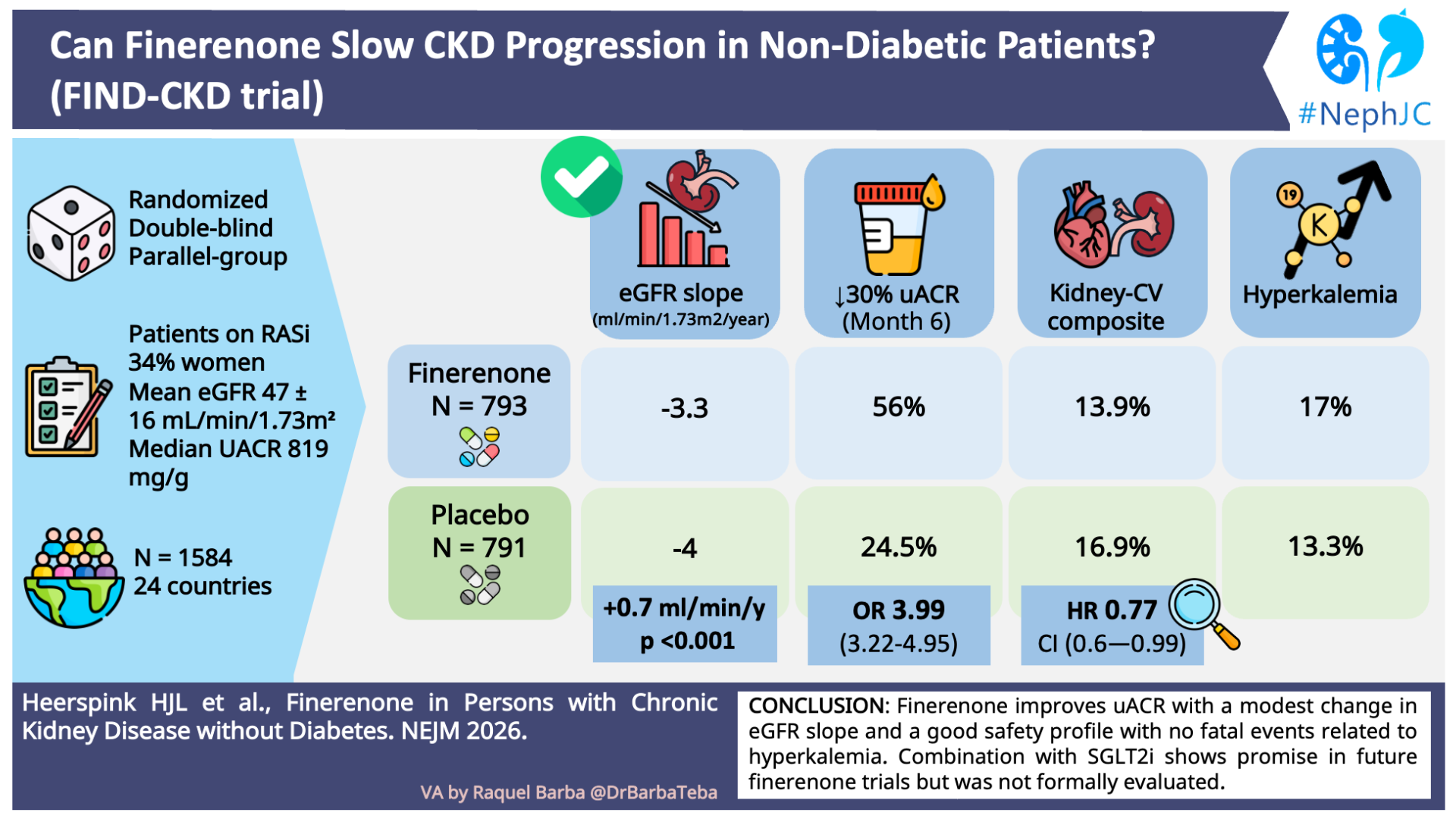
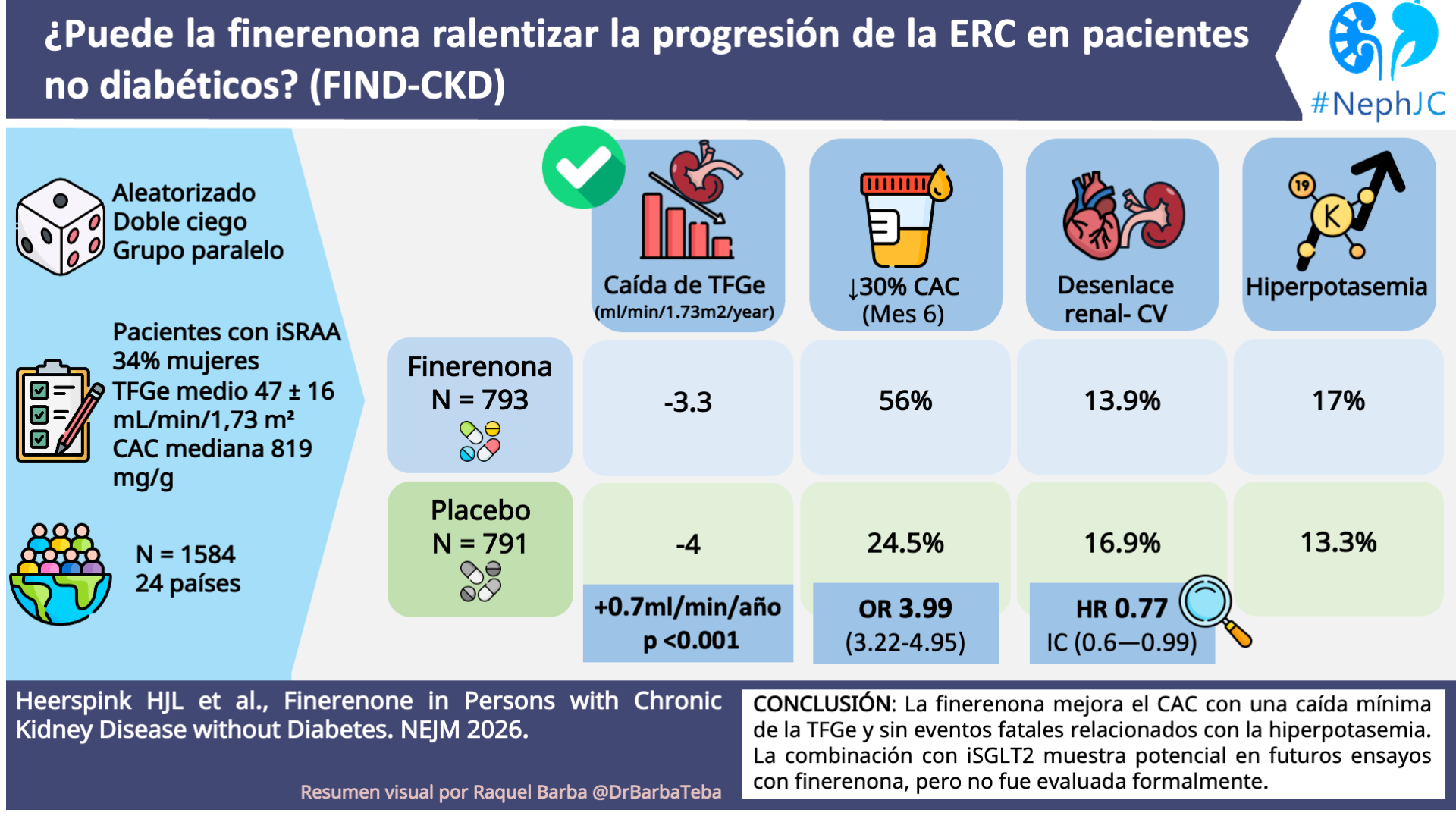
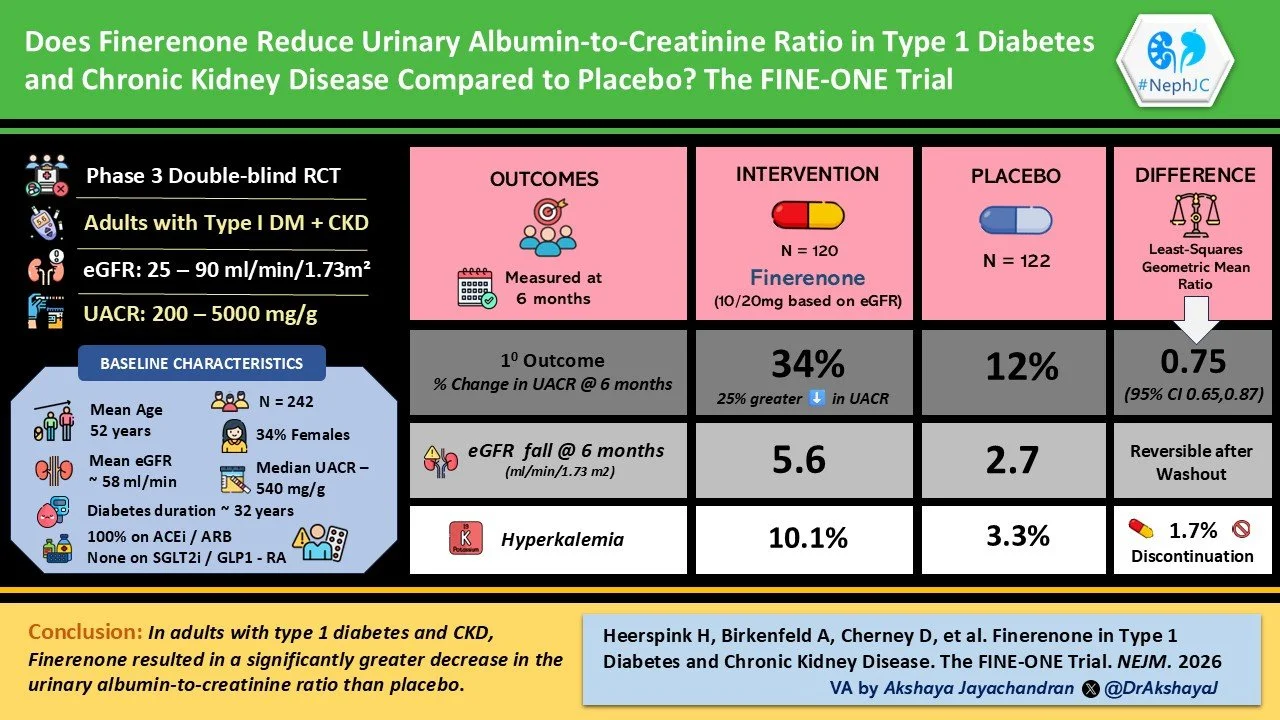
The FINE-HEART pooled analysis has re’FINE’d understanding finerenone’s role as a complementary disease-modifying drug across the spectrum of the CKM syndrome. The role of ns-MRAs in improving kidney outcomes will further be cemented with the upcoming trial FIND CKD (Heerspink et al, NDT 2024) which studied ns-MRAs’ role in non-diabetic CKD and FINE-ONE (Heerspink et al, Diabetes research and Clinical Practice 2023) in type 1 DM. Finally, the upcoming trials CONFIDENCE (Green et al, NDT 2023) and CONFIRMATION HF will throw more light on the combination of ns-MRAs with SGLT2-inhibitor, GLP-1 antagonist therapies. But for now, it is heartening to see ns-MRAs in CKM syndrome are being supported by further large studies in a variety of patients.
Conclusion
Across a wide variety of patients with CKM (with and without CKD, CVD, DM, HF, proteinuria), with varying degrees of severity, finerenone was beneficial at slowing CKD progression and nominally decreased all-cause mortality and heart failure hospitalizations. Overall, ns-MRAs appear to be safe and well tolerated, and should be used in a growing number of patient populations at risk for CVD and CKD.
Summary by Madiha Aziz
Pediatric Nephrologist, Karachi, Pakistan
NSMC Interns class of 2024, Pod 1 Filtrate Firebolts
Reviewed by Brian Rifkin, Cristina Popa, Pallavi Prasad, Sayali Thakare, and Swapnil Hiremath