
NephJC 10 post discussion
Tuesday, June 23rd 2026, 9 pm Eastern on X and Bluesky
N Engl J Med. 2026 Jun 5., doi: 10.1056/NEJMoa2602678. Online ahead of print.
Obinutuzumab or Tacrolimus in Primary Membranous Nephropathy
Fernando C Fervenza, Fan Fan Hou, Chuan-Ming Hao, Gianna M Kirsztajn, Loreto Gesualdo, Tomasz Hryszko, Antonio Pisani, Dario Roccatello, Andrew S Bomback, Julie Rae, Farima Barmaki, Eriola Berisha, Thomas Schindler, Theodore A Omachi, Jay P Garg, Ana Malvar; MAJESTY Trial Investigators
PMID: : 42246654
DOI: 10.1056/NEJMoa2602678





Introduction
If you’re a fan of trying to shoot fish in barrels, then maybe a career in designing obinutuzumab trials is for you. Simply ask ‘Does rituximab work for this condition?’, and then show that obinutuzumab can get the job too - hence the ongoing trials in ANCA vasculitis, frequently relapsing nephrotic syndrome, and this feature - the MAJESTY trial in primary membranous nephropathy (pMN).
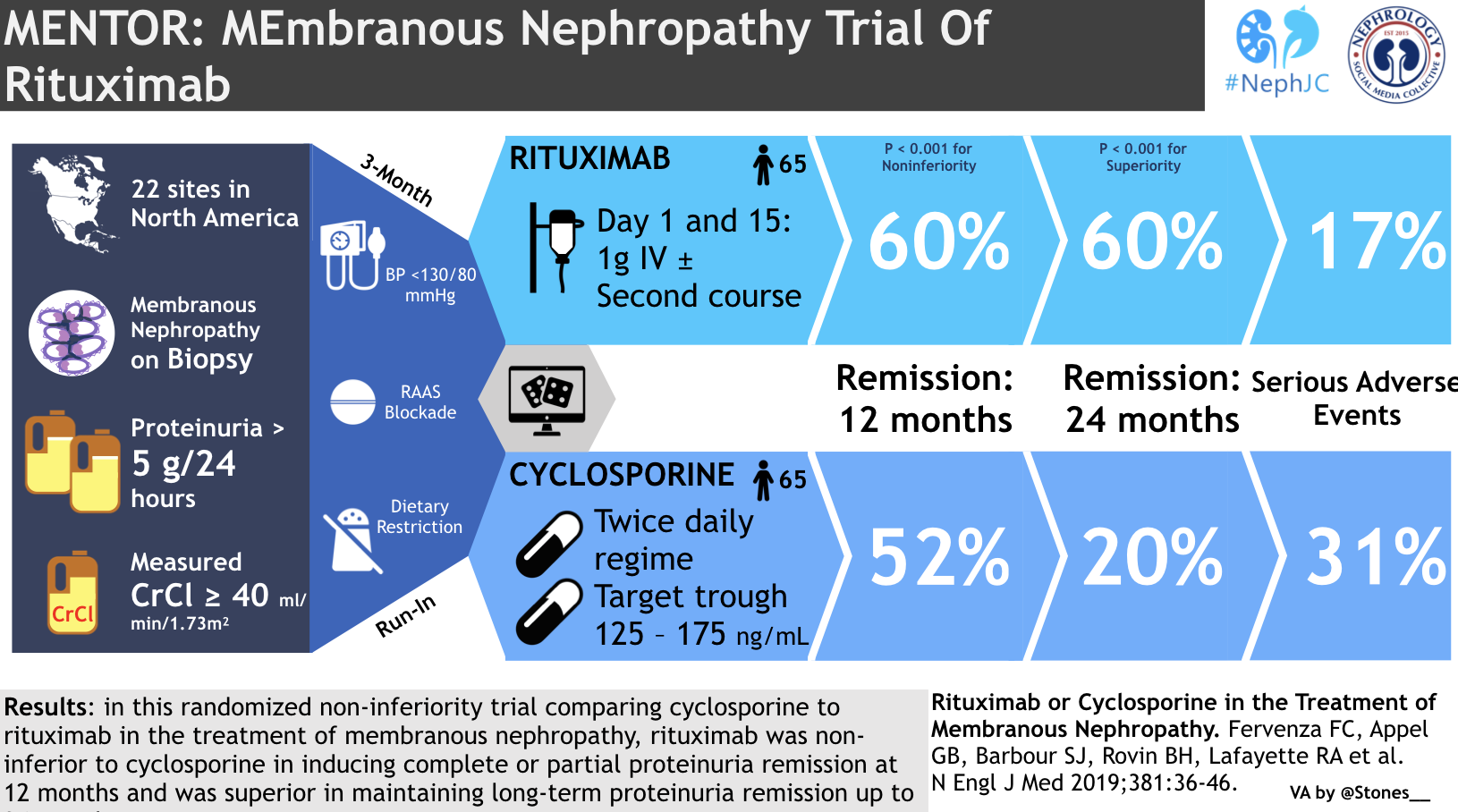
We are well aware that rituximab (RTX) has efficacy in pMN; remember the NephJC summary of the MENTOR trial, in which investigators compared RTX to 12 months of the calcineurin inhibitor (CNI) ciclosporin, and looked at a primary outcome of complete remission (CR) at 24 months. Partly as large numbers of patients relapsed once discontinuing the short-acting CNI, and didn’t relapse when treated with the long-acting RTX, the trial was a significant success for RTX. Even though the sponsor didn’t apply for a label for the indication, ever since RTX has been used off-label by nephrologists with access.
Now the same first author is back for MAJESTY, though the B-cell depletor is swapped to obinutuzumab (OBI) and the CNI is swapped to tacrolimus (TAC). OBI is a type II anti-CD20 monoclonal antibody (whereas RTX is type I), with a glycoengineered Fc region that confers greater antibody-dependent cellular cytotoxicity and direct B-cell apoptosis. RTX, by contrast, relies more on complement-dependent cytotoxicity and is more prone to CD20 internalization, a potential resistance mechanism. These differences translate into more profound and sustained B-cells depletion with OBI, including superior clearance from peripheral sites like lymph nodes and spleen (Mossner E et al, Blood, 2010| Reddy V et al, Rheumatology, 2017). OBI’s first trip to NephJC got it off to a very good start, as though LUNAR was negative (with caveats) for adding rituximab to standard of care in lupus nephritis, OBI in the REGENCY trial was actually able to show nice additional benefit. It has been around for over a decade for the treatment of chronic lymphocytic leukeamia (CLL), but then excitingly also recently gained a license for lupus nephritis, and case reports about OBI efficacy in treatment-resistant cases of almost all of our immune-mediated kidney diseases continue to grow.
CNIs reduce proteinuria partly via hemodynamic effects (afferent arteriolar vasoconstriction) without necessarily inducing immunologic remission, contributing to high relapse rates after withdrawal - unlike B-cell depleters, that target the autoantibody source (Faul C et al, Nat Med, 2008).
In pMN we have already had case series such as this one of 20 ‘RTX-resistant’ patients with pMN who were given OBI, with encouraging results (Su X et al, KI reports, 2024). There is also an ongoing need in first line therapies in pMN, as currently a substantial proportion of patients fail to achieve complete response, remission occurs slowly (especially in those with very high starting PLA2R titres), and relapses occur - this has set the stage to see what would happen when more potent B-cell depletion strategies are used up front rather than just in a resistant cohort.
The Study
Methods
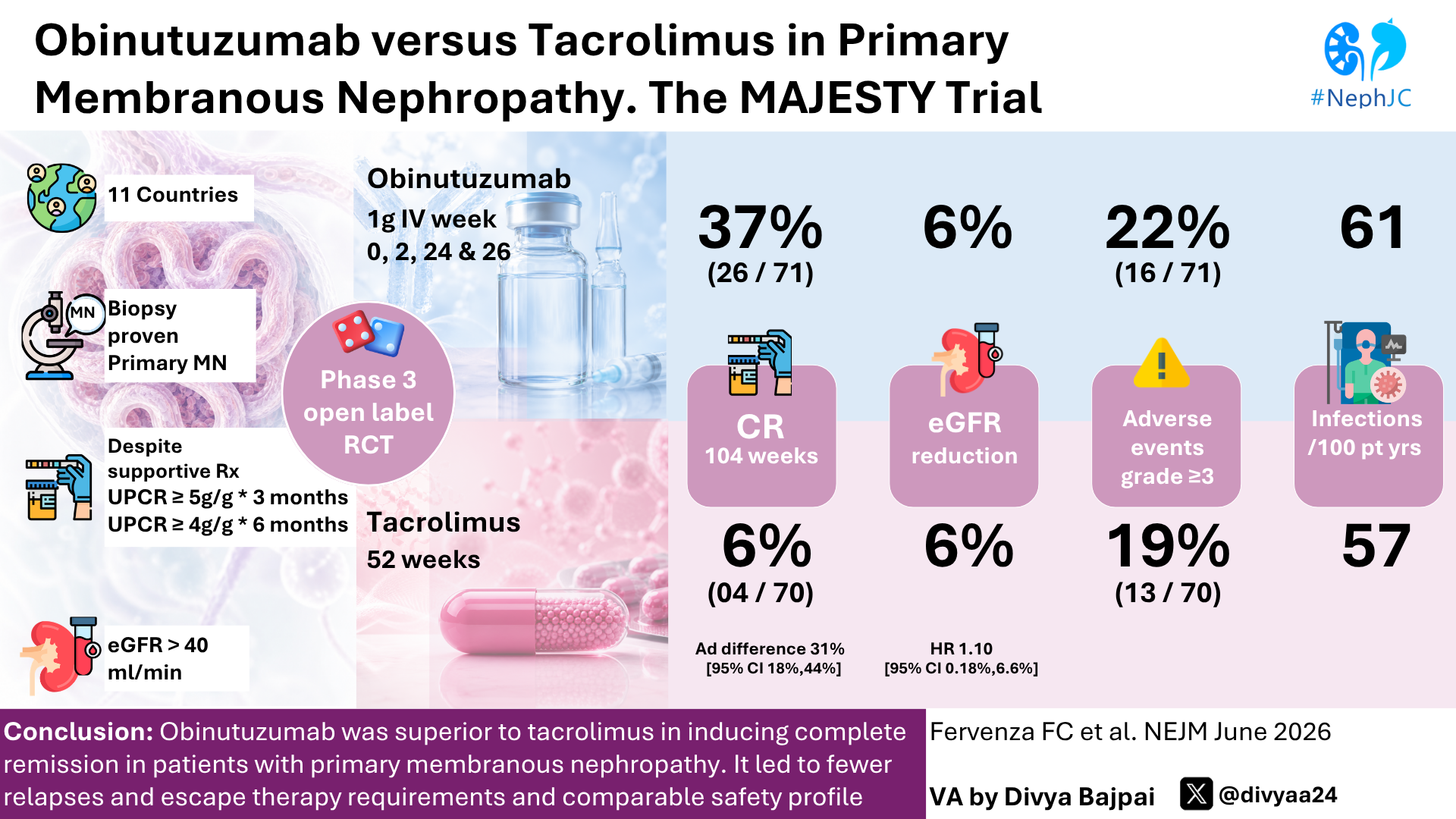
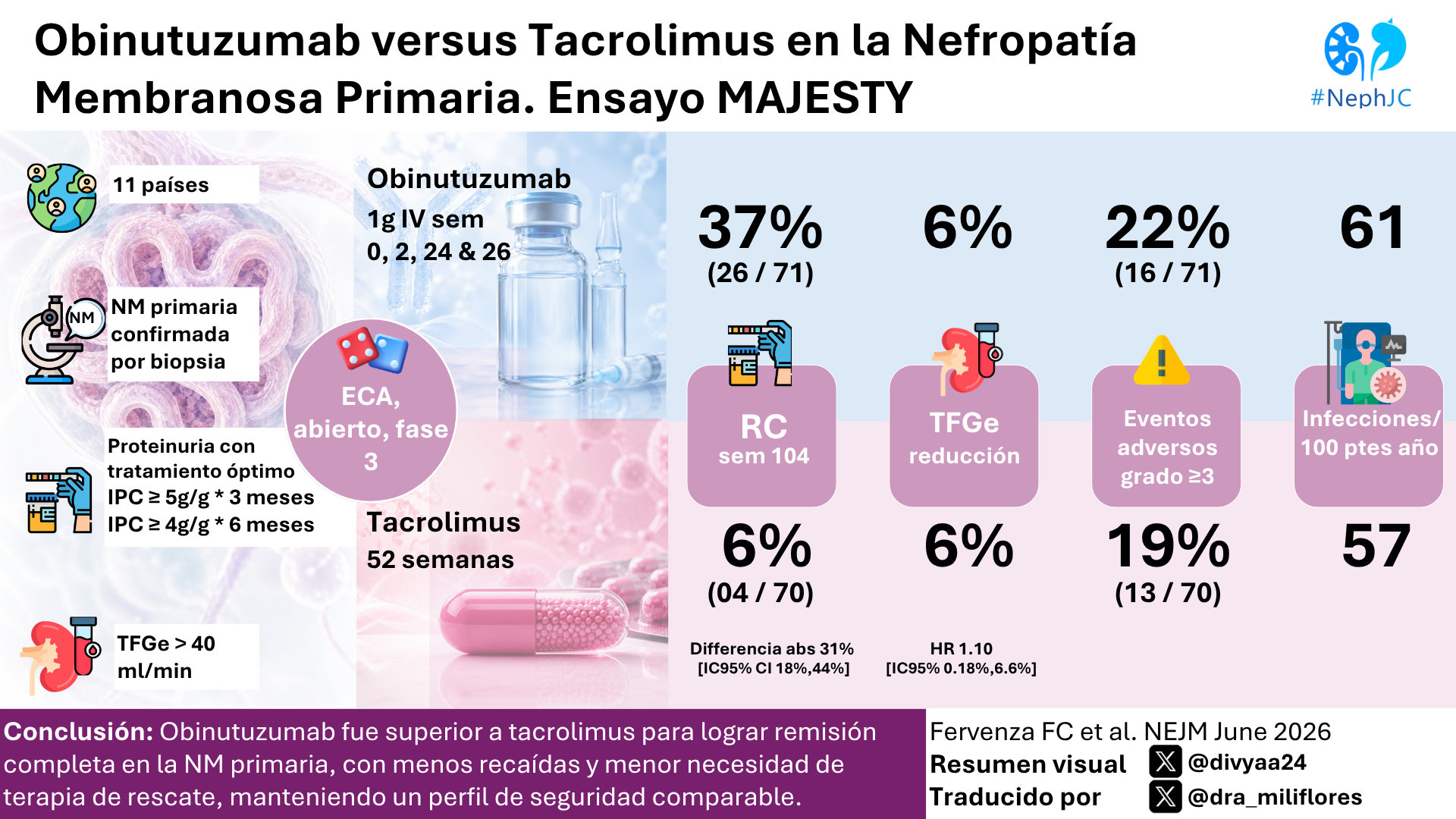
MAJESTY was a multinational, randomised, open-label, phase 3 trial of obinutuzumab against tacrolimus, conducted at 49 sites across 11 countries.
Inclusion criteria
Adults aged 18–75 years with all of:
Biopsy-proven, primary membranous nephropathy
Persistent nephrotic-range proteinuria despite optimized supportive therapy
uPCR ≥5 g/g (>565mg/mmol) for at least 3 months, or
uPCR ≥4 g/g (>450mg/mmol) for at least 6 months
eGFR ≥40 mL/min/1.73 m²
Patients previously treated with immunosuppression could be included, provided at least 6 months has passed since they’d had CNI or cyclophosphamide, or 9 months for RTX, and they’d not demonstrated resistance to RTX or CNI in the past. Other exclusion criteria included evidence of spontaneous remission, diabetes, or suspected secondary MN.
Randomisation
Patients were randomised 1:1 to receive open label:
Obinutuzumab
1000 mg IV at day 1, week 2, week 24, and week 26
or
Tacrolimus
Starting dose 0.05 mg/kg/day, in 2 divided doses
Trough target 5–7 ng/mL
Maintained through week 52 (unless complete proteinuria response, in which case tapering could start from week 36)
Tapered over 8 weeks
Randomisation was stratified by region, and anti-PLA2R antibody level (≥175 U/mL vs lower).
If patients met pre-defined failure criteria in either arm there were 4 time points at which their treatment would change, as below, which they called ‘escape criteria’:
Primary endpoint
Complete remission (CR) at week 104, defined as::
uPCR ≤0.3 g/g (<34mg/mmol) on 24 hour urine collection, AND
Stable kidney function (eGFR ≥85% of baseline), AND
No intercurrent events (escape therapy, treatment failure, early study withdrawal)
Key secondary endpoints (tested in hierarchical order)
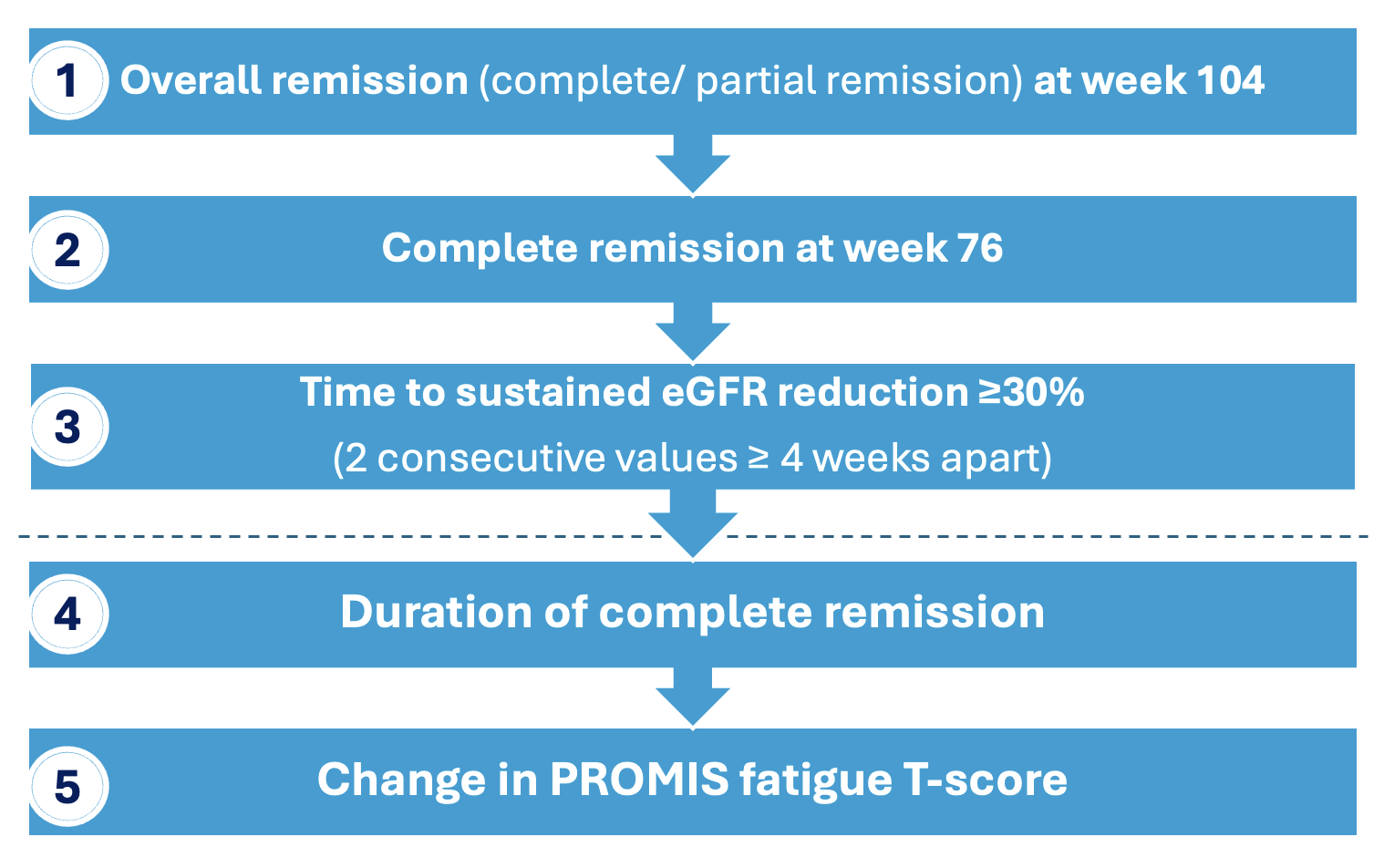
Partial remission (PR) was defined as a 50% reduction in uPCR from baseline but still in the 0.3 - 3.5g/g range (35 - 396mg/mmol) AND with stable eGFR.
Specifically based on MENTOR, they estimated that a sample size of 140 patients would provide the trial at least 90% power to detect a difference between trial groups in the percentage of patients who had complete remission (25% with OBI vs. 5% with TAC) at a two-sided alpha level of 0.05. The efficacy analyses were performed in the intention-to-treat population, which included all the patients who had undergone randomisation, with patients grouped according to the treatment assigned rather than the treatment received.
As seen in Figure S1 above, there is a study of longer term safety planned for a further 2 years, the results of which are not yet available.
Funding
The sponsor (Roche) designed the trial, participated in the collection, analysis, and interpretation of the data, and contributed to manuscript preparation - with their employees amongst the authors.
Results
The consort diagram is found in figure S2:
Fig 2 Consort Diagram. Fervenza FC, et al. N Engl J Med, 2026.
The baseline characteristics are shown in Table 1:
Table 1. Patient Characteristics. Fervenza FC, et al. N Engl J Med, 2026.
Of note, the population had a mean age of 50 years with male and white pre-dominance, and around 78% PLA2R positivity, all of which is representative of pMN. Mean eGFR was >80, and mean 24 hour urinary protein level was around 10g/day despite great uptake of RAASi, with mean serum albumin of 29. Around 30% had received prior immunosuppressive therapy. Rates of supportive care with baseline SGLT2i were not reported (and their addition was not permitted during the trial).
Slightly confusingly, the eGFR range seems to go down to 24 mL/min/1.73 m² in Table 1, and the uPCR range down to 1.7g/day, making it unclear how these patients were recruited, as these values fall outside the inclusion criteria (our assumption being their lab values changed between screening and first visit).
Primary Endpoint
The trial met its primary endpoint convincingly - at week 104, 37% of patients in the OBI group had reached complete remission (CR), versus only 6% in the TAC arm, which (as you’d guess) was highly statistically significant.
Fig 1. Complete remission. Fervenza FC, et al. N Engl J Med, 2026.
Analysis showed consistent results across all sub-groups.
The peak remission rate with obinutuzumab occurred by week 76, and was sustained thereafter. For key secondary endpoints: overall remission at week 104 was 51% vs 13% (P<0.001), and complete remission at week 76 was also significant (44% vs 14%). Patients on TAC who had achieved CR/PR relapsed very frequently after drug weaning at 52 weeks, as shown in Figure 2.
Fig 2. Relapses after CR/PR. Fervenza FC, et al. N Engl J Med, 2026.
Sequentially next, the sustained eGFR reduction endpoint showed no difference (6% in both arms; HR 1.10, 95% CI 0.18-6.61), at which point hierarchical testing stopped. Consequently, the duration of CR and PROMIS fatigue score changes were not formally tested and their CIs are descriptive only (though the fatigue scores don’t appear to have a meaningful clinical difference).
Escape Therapy
A vast majority (61%) of the TAC arm met escape criteria and therefore received OBI, with what appears to be a reasonably even split between meeting escape criteria during the first or second year of the study (with 10 patients at week 24, 3 at week 52, 17 due to relapse after week 52, and 9 due to increased serum creatinine while on TAC). In the OBI arm 28% met escape criteria (meaning that 44% of the entire trial population met escape criteria at some stage). Data on total OBI doses given across the original arms and then in the escape groups was not reported. Only 2/70 patients in the OBI arm had to start an additional non-glucocorticoid immunosuppressant due to treatment failure.
Immunologic remission and B-cell depletion
Immunological remission (defined as a change in anti-PLA2R autoantibody status from positive to negative) can of course only be explored in PLA2R positive patients. As can be seen in Figure S6(A), OBI gave faster, more effective, and more sustained PLA2R suppression when compared to TAC, with consistent results seen even when looking at patients with high starting PLA2R titres (defined here as ≥175 U per milliliter).
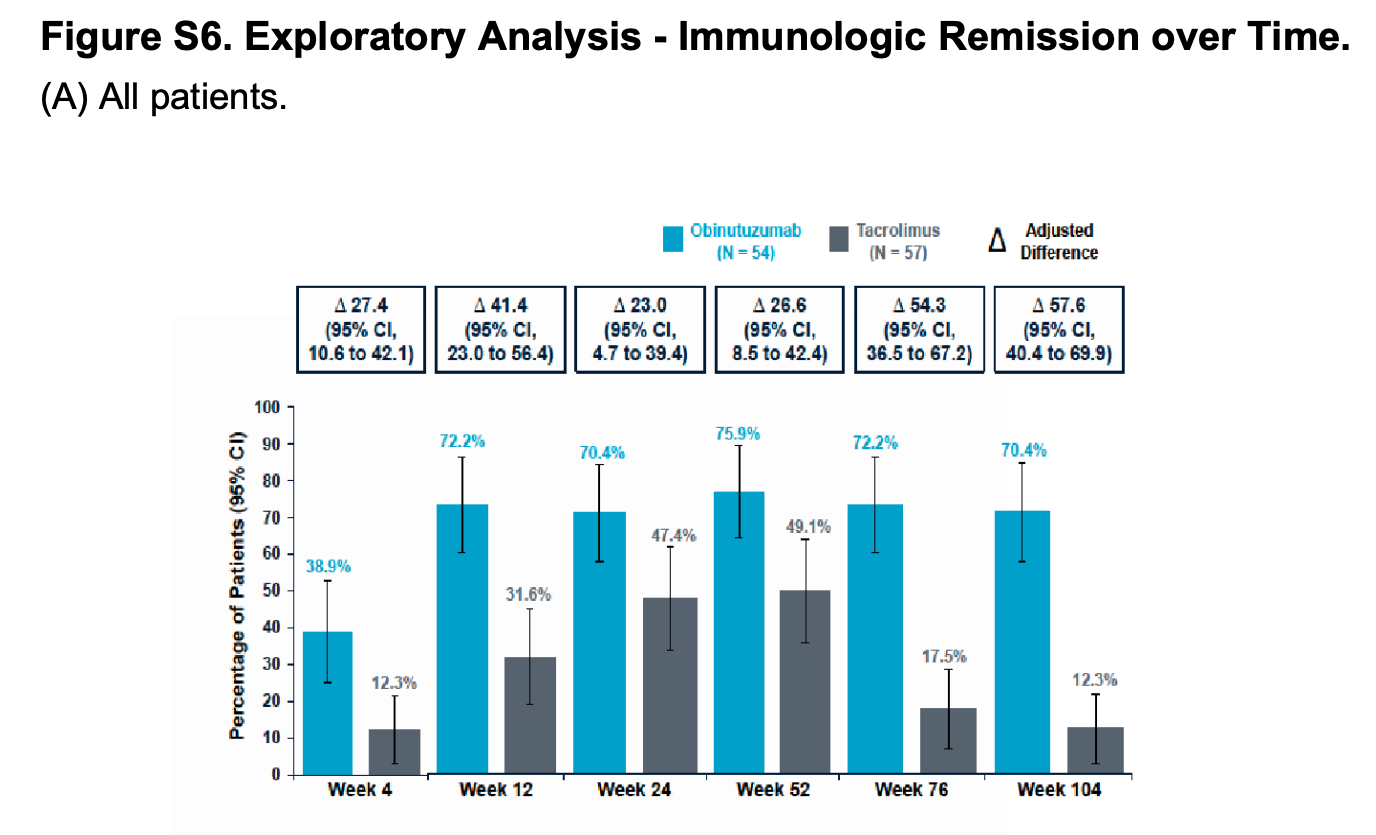
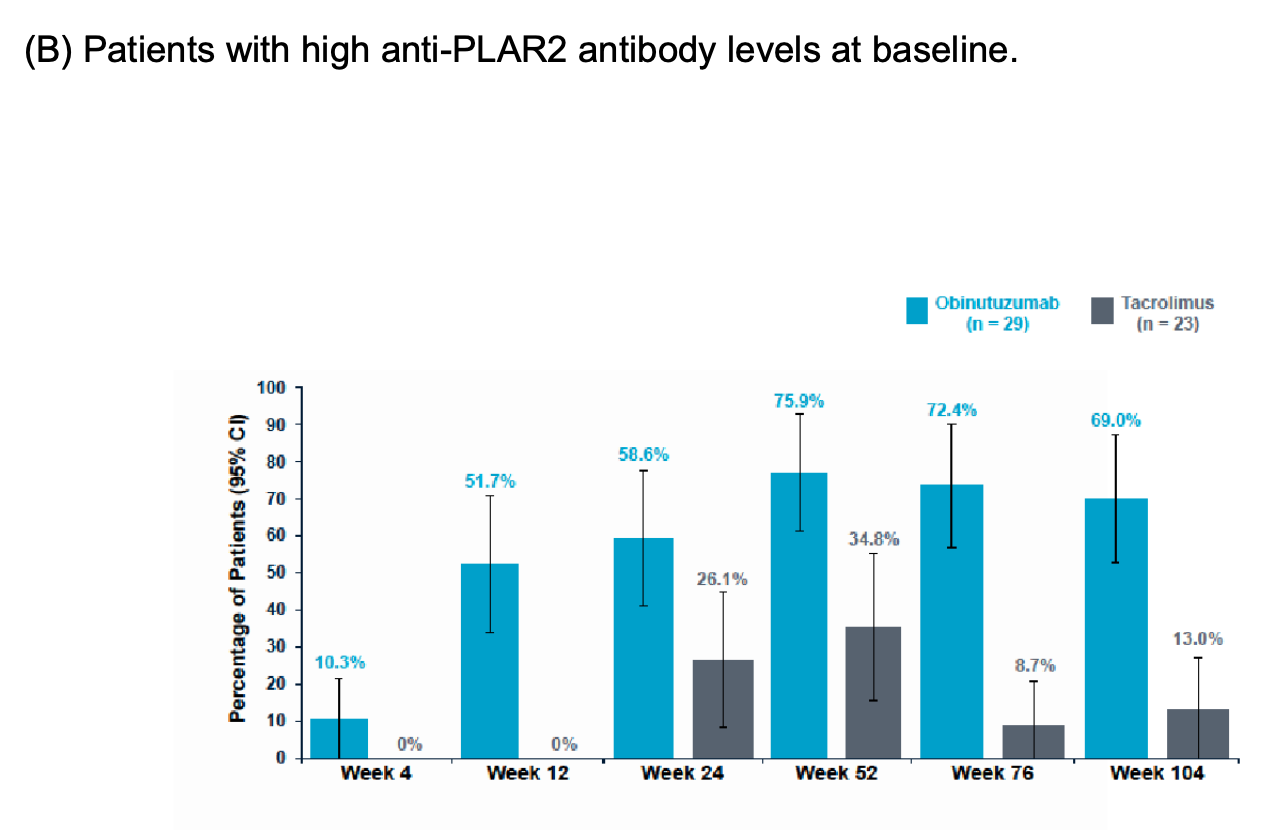
Fig S6 A/B. Immunologic remission of anti-PLA2R. Fervenza FC, et al. N Engl J Med, 2026.
OBI certainly does what it says on the label - depletion of CD19+ B cells seen in Figure S8(A).
Fig S8. CD 19+ B-cell depletion. Fervenza FC, et al. N Engl J Med, 2026.
The pattern of complete B cell depletion (levels <10 cells per microliter) is interesting, tailing off a little before the second course of OBI was administered at 6 months, getting to 94% of the patients with complete depletion at week 52, which gradually dropped to only 14% by week 104. Notably, the protocol defined depletion as ≤5 cells/ microliter, and no justification for this threshold change compared to protocol was offered.
Fig S8 B. Proportion of patients with CD19+ B-ce;;s < 10 cells/µl. Fervenza FC, et al. N Engl J Med, 2026.
Safety
The analysis of any safety signals gets a bit hard to interpret and needs some background knowledge to read - Table 3 reports the randomised safety data for the 104 week trial, but not if they left, as directed for escape therapy. Therefore, what you are seeing in Table 3 is NOT safety data for all the patients who received OBI (remembering that 61% of the original TAC group met escape criteria and then received OBI). In fact, no systematic escape period safety data are reported anywhere. At a glance, you might think no deaths occurred, but actually, as is explained in the legend, two deaths did occur during escape therapy with OBI (one from each original treatment arm), attributed to covid-19 pneumonia and cardiac arrest. The main article text states that investigators did not think the pneumonia death was related to the OBI received (though how exactly one adjudicates a death due to infection as unrelated to the potent long-acting B-cell depleter you have given them is not justified further, especially given deaths due to covid-19 were much less common by the time recruitment opened in summer 2021).
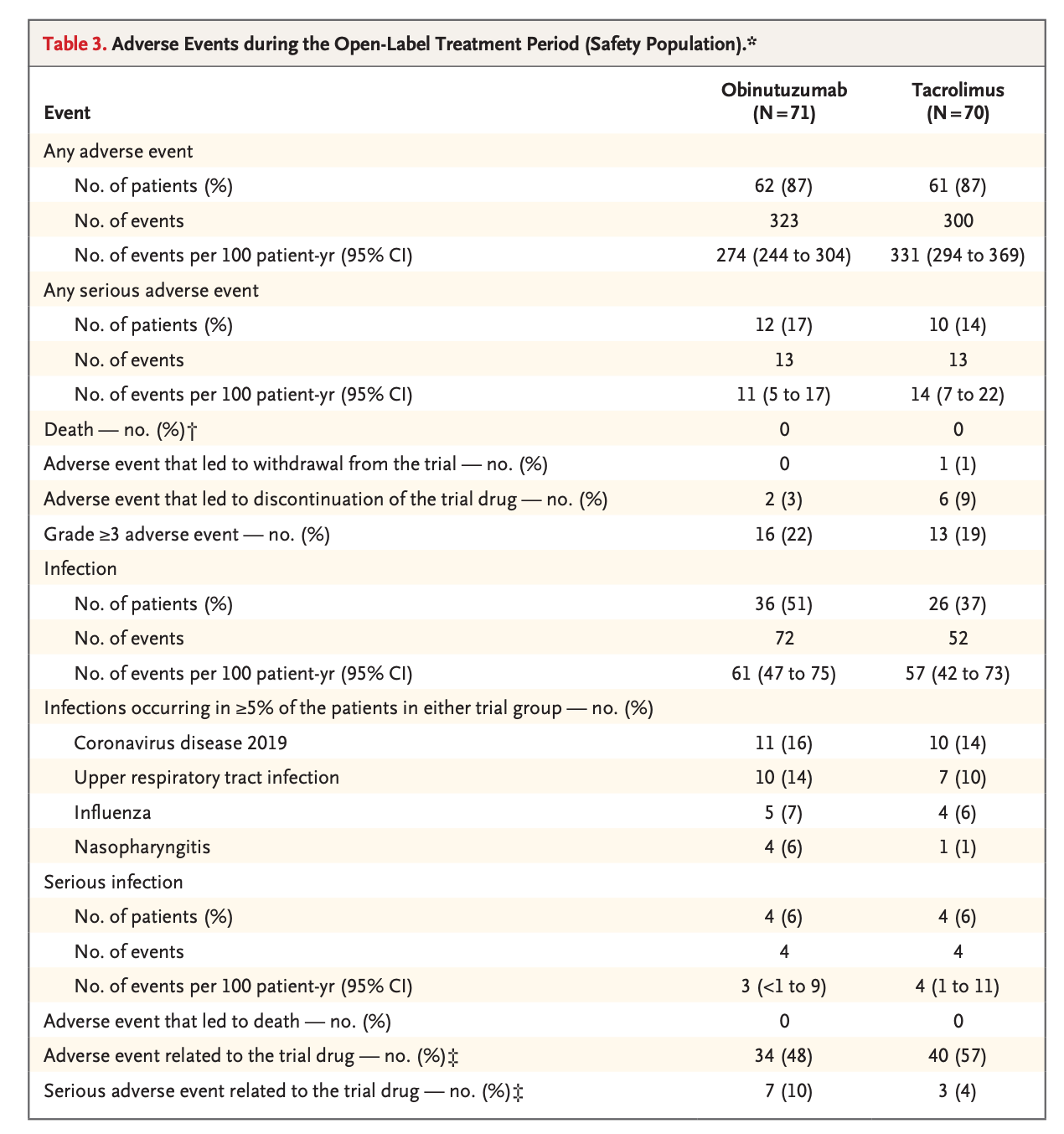
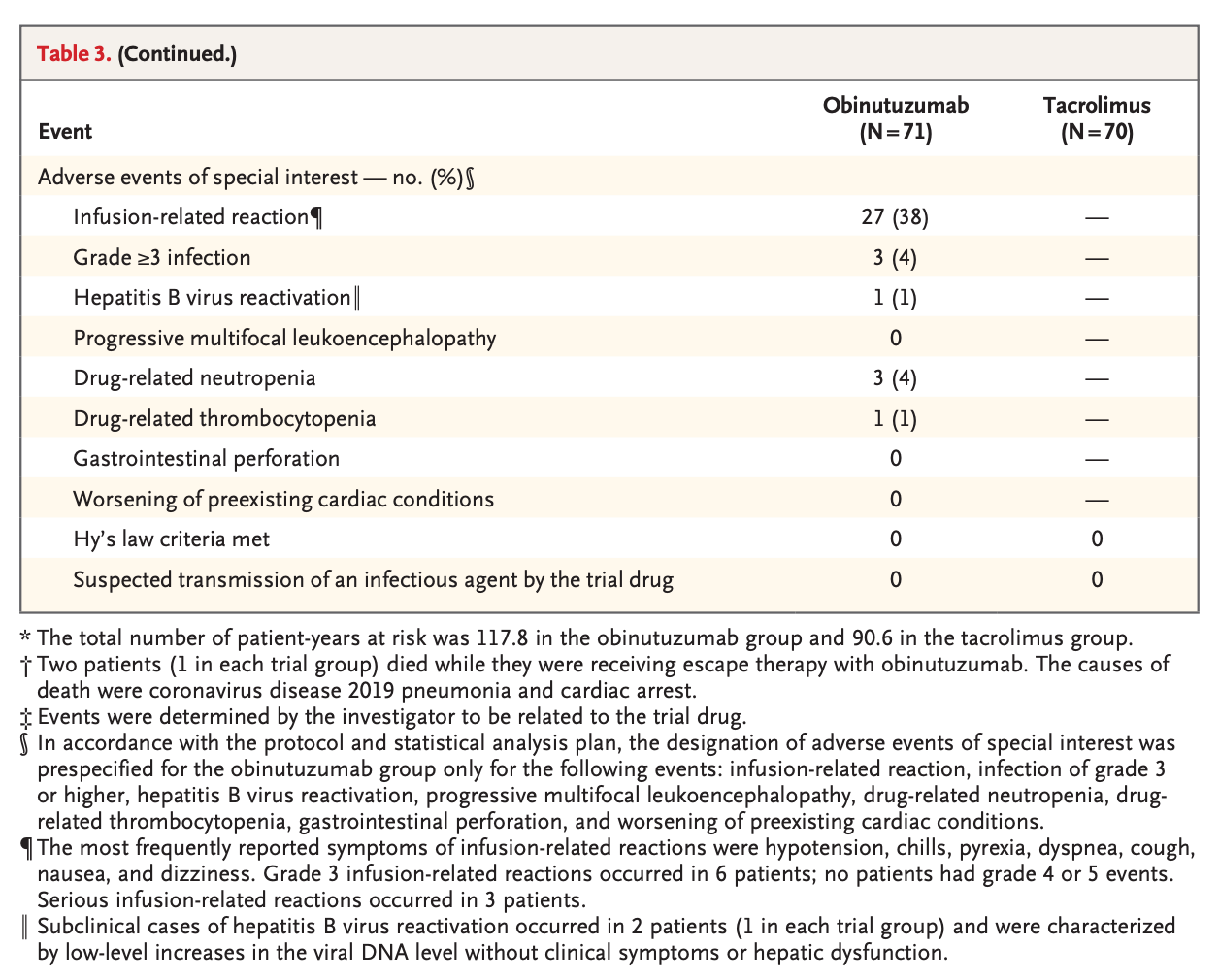
Table 3. Adverse events. Fervenza FC, et al. N Engl J Med, 2026.
Infections occurred at a rate of 61 events per 100 patient years in the OBI arm and 57 per 100 patient years with TAC. Serious adverse event rates per 100 patient-years were 11 (OBI) vs 14 (TAC). Table 3 reports a 4% neutropenia rate with OBI, though the relevance of this is less clear when overall the infection comparison data is reassuring.
There was a 38% infusion reaction rate with OBI, but they specifically note that these were manageable with infusion-rate adjustments and symptomatic treatment. I think we’d interpret Table 3 and it’s legend as saying two subclinical HepB re-activation events occurred, one in the OBI arm and maybe one after OBI was given for escape criteria (as if re-activation occurred on TAC it would be recorded in Table 3, which it is not) - it is unclear, and it’s also not stated whether the re-activation occurred despite antiviral prophylaxis or not.
The number of patients in both arms who had a sustained eGFR decrease of >30% at week 76 was low, at 6% in both arms.
Serum IgG levels actually increased over the course of the trial in both arms, likely due to decreased IgG losses in the urine as nephrosis improved, and not indicating less IgG recovery with OBI over TAC.
Fig S11. Immunoglobulin concentration over time. Fervenza FC, et al. N Engl J Med, 2026.
Discussion
MAJESTY results analysis
No one is surprised to see the pattern of MENTOR’s results reproduced here 7 years later - patients who stop their CNI then frequently relapse over the next year, whereas the patients who instead received long-acting B cell depletors are much more likely to achieve and stay in remission.
It is nice to see not only that OBI works in a large cohort, but in particular the immunological remission data looked impressive. There was no difference in renal function between groups, as would be expected over a 2-year follow-up of a group with relatively preserved kidney function at baseline.
The catchphrase of seemingly all Phase 3 trials presented at ERA was ‘there were no new or unexpected safety signals’. Equal infection rates between arms looked reassuring, as did the IgG data, but given there is a black box warning regarding hepatitis B reactivation on OBI’s FDA prescribing label, I don’t think it is too much to ask for them to be more explicit on whether the 2 patients who had subclinical HepB reactivation during the trial had both had OBI, as the text leaves you guessing. Rates of neutropenia of 4% with OBI were lower than the 14% seen in REGENCY (Furie RA et al, NEJM, 2025), probably because these patients with SLE were also on MMF, and in keeping with this, the placebo control arm in REGENCY also had high neutropenia rates at 6%. They do make it clear in MAJESTY that both patients who died during the trial had received OBI, even mentioning this in their abstract. As in REGENCY, a death due to COVID-19 after OBI in this trial could be seen as a marker of increased viral morbidity, though somehow here the investigators judged the COVID-19 death and having received OBI as unrelated to each other, which, at face value, is baffling. The supplement in REGENCY gave further details about deaths, but no further details were given here. It also appears the local investigators have flagged up more ‘adverse events related to the study drug’ in the TAC arm than with OBI, with 34 events in the OBI arm - though with 27 infusion reactions and 36 patients having infections in the OBI arm, it isn’t clear how that maths stacks up, and it’s just hard to see how an investigator could confidently judge an infusion reaction or infection to be unrelated to their open label B-cell depletor immunosuppression. Very disappointingly, there is also a major safety reporting gap of adverse events during escape therapy, with no mention of infusion reaction or infection rates for the large crossover population, which you’d have thought would have been common sense to include.
Comparison with MENTOR and rituximab
OBI isn’t trying to inherit the throne from CNI therapy in countries that will be able to afford OBI access - it’s trying to succeed rituximab. While MAJESTY was obviously not designed to test whether OBI is superior to rituximab, and comparing different trials must be done with caution, nephrologists will still be tempted to compare results here with those from MENTOR (Fervenza FC et al, NEJM, 2019).
Inclusion criteria were similar enough, and baseline characteristics of the population were also broadly similar. MENTOR and MAJESTY differed in their exact outcome definitions, in that MAJESTY more stringently also required eGFR preservation ≥85% of baseline in both their CR and PR definitions on top of proteinuria remission, whereas MENTOR had proteinuria criteria only. In that context, looking at CR at week 104, it was 37% in MAJESTY with OBI versus 35% in MENTOR with RTX. In MAJESTY at week 104 CR and PR combined was only at 51% with OBI, whereas it was up at 60% with RTX. However, if the eGFR criteria were removed from the MAJESTY definition and instead just the proteinuria definitions were applied to both, then at 52 weeks, OBI CR rates were 26% versus 14% in MENTOR, and by week 104 OBI got 49% to complete proteinuric response versus the 35% in with RTX.
‘Reading the tea leaves’ of the above, you could say that OBI’s results look better than the RTX results, if not dramatically so. It’s not clear why the eGFR criteria for PR/CR were added between studies.
What about the patients with high starting PLA2R titres? To remind you of table S13 from MENTOR, when they split their patients into tertiles of PLA2R level, the immunological response rate did tail off a lot in their highest PLA2R cohort, unlike OBI’s results here (accepting the number of patients in each group by that stage of subdivision is relatively small).
In terms of safety, MENTOR did not include neutropenia or IgG data, and did report that RTX had numerically fewer infection events than ciclosporin. They did not have any deaths during the trial, which is the norm across pMN trials, and contrasts with MAJESTY. Infusion reactions to RTX were at 25% (which certainly seems higher than I’d have expected), versus the 38% rate with OBI.
MAJESTY limitations
The open-label design certainly risks influencing more subjective outcomes like ‘AEs related to study drug’ and fatigue score, if less so the hard ‘number based’ outcomes of the trial, and blinding would have been difficult (given the high rates of transfusion reaction and need to adjust TAC doses based on levels) and time-consuming. Treatment durability and safety beyond 2 years is currently unknown, and the further 2 years of observation is underway.
However, the big talking point of MAJESTY will be the decision to have the comparator as 52 weeks of TAC, rather than against RTX. In recent years, we’ve been inundated with trial designs that aren’t exactly what patients or their doctors would have chosen - voclosporin not being compared to TAC for lupus, or finerenone against other MRAs, to name a few - and here finding that B cell depletion therapy beats 52 weeks of CNI at a 104 week endpoint was certainly not providing the world with new scientific information.
Supporting the choice of TAC in MAJESTY is that 7 years ago a study of US prescribing patterns still put TAC use at 40% (O'Shaughnessy MM et al, Kidney Int Rep. 2019), though you’d expect this to have shifted significantly since MENTOR, and the fact that TAC is on the KDIGO GN guidelines (at least for patients at moderate risk, though you’d guess actually many MAJESTY patients actually fell into the high risk group, in whom KDIGO would not have recommended CNI - I’m looking at that 3043 U/ml PLA2R titre in Table 1…). But most importantly, the increase in sample size that would have been required for a superiority trial of OBI versus RTX would have been entirely prohibitive, put at n=2500 patients if assuming 45% versus 35% remission rates, which can’t be done in rare disease. The ‘need’ to have a feasible trial done has been said to be that it is hard to access RTX in the US given the lack of license for the pMN indication, whereas now hopefully OBI will soon be licensed - though anecdotally plenty of US physicians do seem to access RTX without any problems as things stand.
The escape criteria were enacted to standardise the implementation of an effective rescue therapy - interestingly, the initial protocol had TAC as the switch option for patients failing on OBI, but this was replaced in later iterations by a second course of OBI, which seems reasonable. The large breadth of the escape criteria was important, as investigators knew patients randomised to the TAC arm were going to relapse like wildfire when they discontinued the TAC at 52 weeks in the same way that occurred many years prior in MENTOR, but the huge 61% of patients on TAC meeting escape criteria did make this trial feel almost closer to a cohort study of OBI rather than an RCT of two effective therapies. The primary estimand’s composite strategy (counting escape as non-response) correctly penalizes the TAC arm, preserving intent-to-treat validity. However, the treatment policy sensitivity analysis (counting escape responses) showed a similar effect (44% vs 14%), confirming robustness (table S5).
MAJESTY’s TAC monotherapy arm contrasts with STARMEN’s (Fernandez-Juarez G et al, Kidney Int, 2021) sequential TAC-RTX regimen (58% CR/PR at 24 months). The 20% CR/PR rate in MAJESTY’s TAC arm at 24 months is far lower, confirming that adding RTX at TAC withdrawal (as in STARMEN) prevents relapse, but still likely underperforms OBI monotherapy (accepting that in clinical practise most would add the RTX earlier than in the STARMEN protocol in the hope of improved outcomes).
The question is, would you let your family member be recruited into a trial in which, by their own numbers, they (accurately) predicted a primary outcome achievement rate in one arm of 5%, when a much more effective therapy exists? To be fair, relapse is not a disaster in pMN when the patient is closely watched, but would you risk randomisation to TAC if their eGFR was 40 and proteinuria >10g/day? I’m really not so sure. However, if you were hoping this is the last pMN trial of ‘new agent versus CNI’ then you haven’t heard of the Phase 3 PROMINENT trial of felzartamab versus TAC with completion expected in 2029, or the Phase 2/3 ALMOND trial of zanubrutinib versus TAC also on the horizon - so it looks like we’re getting everything compared to TAC (except, of course, for voclosporin) for a while yet. How we’ll sort out which agent is best in 5 years when they have never been directly compared to one another is anyone's guess for now, but the industry interest in pMN will hopefully be a great thing for patients going forward.
Will clinicians now use OBI first line?
It is accepted that OBI has superior speed and depth of B-cell depletion compared to RTX, particularly in lymph nodes and spleen; for the simple-minded like me, it can be thought of as ‘super-rituximab’, much like sparsentan for IgAN sits in my brain as ‘super-ACEi’, with increased efficacy but also concern regarding an uptick in side-effects that goes along with that. While waiting to see if OBI gets approval for pMN in their healthcare system, nephrologists will meanwhile gain experience with OBI from the lupus nephritis indication, and we’ll be eager to see more and more trials in disease areas where RTX is good but there’s room for improvement, for example, in this phase 2 in AAV, which, fantastically, they have finally called OBI-WAN.
Now, on top of the reports that OBI can overcome the pMN disease that is resistant to RTX, we have this MAJESTY data, which indicates an impressive immunological response even in patients with high starting PLA2R titres (which may be lacking with RTX), and likely favourable proteinuria outcomes at 2 years with OBI compared to what RTX achieved in MENTOR. If access to both were equal, you can imagine many reaching for OBI first line now if their patient is in agreement, though the safety data outlined above may put some off. If having a license for the pMN indication makes a huge difference to access in an insurance-based system, then first-line OBI will become the norm in those areas, whereas in systems which (forgive me) sensibly recognise the rituximab efficacy data and prioritise value over formal application for indication, then it seems possible that OBI will be rationed in some healthcare systems only for resistant patients, especially with generic RTX now available. Of course, some clinicians will want to reach for OBI in patients with high PLA2R titers, but others might make do with RTX in combination with a few early months of CNI for their higher-risk patients, or give more doses of RTX than usual in the hope of deeper B-cell depletion. Overall, it will be good for patients to have increasing options, and the toxicity of cyclical cyclophosphamide/steroid protocols will be seen less as treatment resistance is increasingly consigned to the past.
Conclusion
MAJESTY had no surprises by showing obinutuzumab beats 52 weeks of tacrolimus in primary membranous, with markedly fewer relapses and escape-therapy requirements.
No doubt a label application will come and be successful, and then we’ll constantly hear how obinutuzumab is “the only licensed treatment for membranous nephropathy”. For the future it’s great that patients will have increasing options with additional efficacy, but if where you work still has you reaching for rituximab rather than obinutuzumab for now, on balancing the available efficacy and safety data it seems unlikely your patients are missing out too much.
Written by Jamie Willows
Renal and GIM Consultant
South Tyneside and Sunderland Foundation Trust
UK
Reviewed by
Joel Topf, Cristina Popa, Brian Rifkin, Pallavi Prasad
Audiosummary prompted by Nikhil Shah
Header designed by AI and prompts from Brian Rifkin