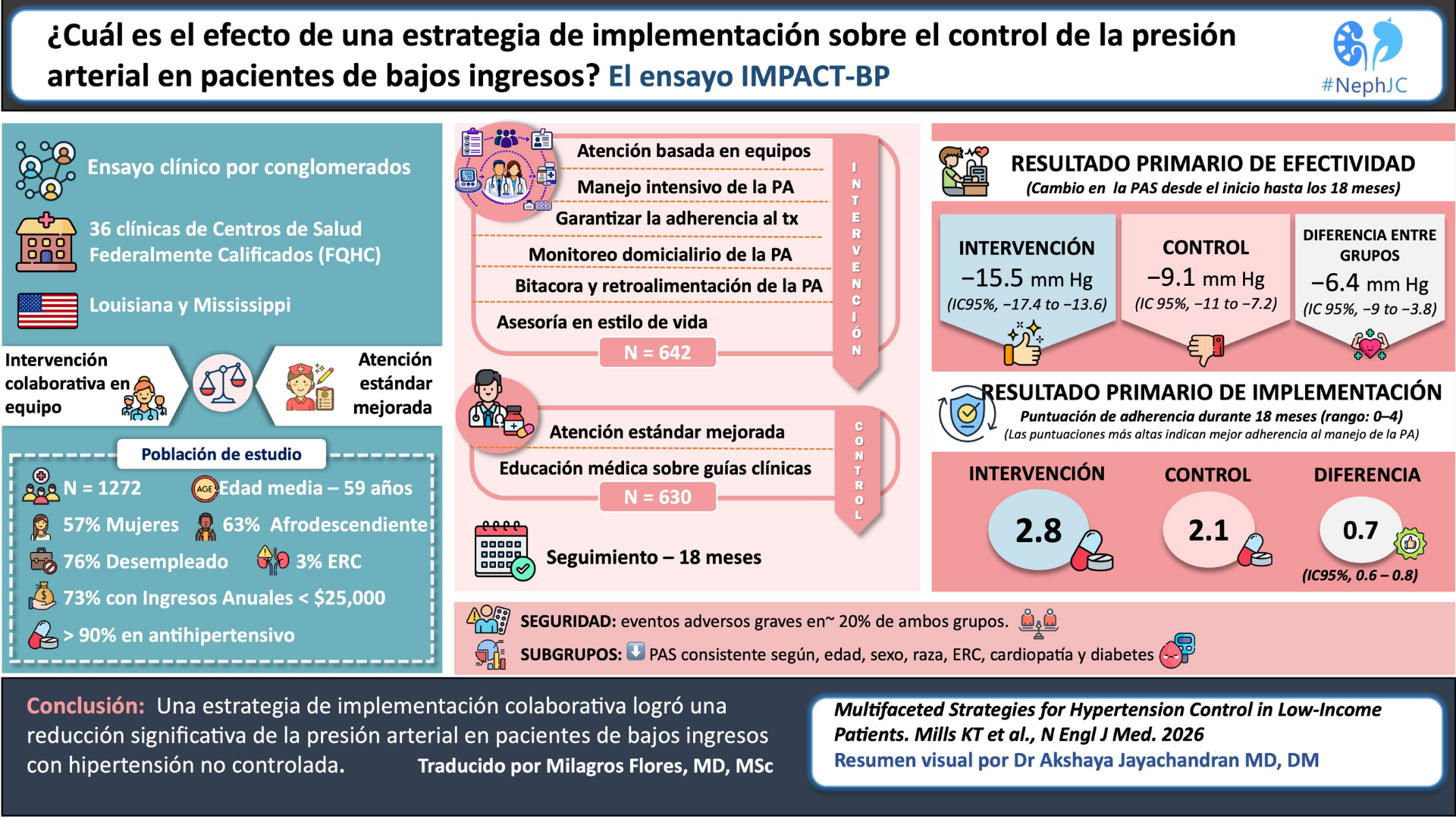


This week we will discuss whether a bundled, team-based hypertension intervention- featuring intensive BP targets, home monitoring, health coaching, and audit feedback- can overcome poverty, clinical inertia, and fragmented care to improve blood pressure control in low-income patients receiving care at federally qualified health centers.